

Summary
Rheumatic diseases are associated with a known risk of premature cardiovascular disease. This article not only discusses best practices, but also the prevention and management of cardiovascular risk in patients with inflammatory disorders.
- rheumatoid arthritis
- inflammatory disorders
- coronary artery disease
- lupus
- rheumatological autoimmune disorders
Rheumatic diseases are associated with a known risk of premature cardiovascular disease (CVD). This Best Practice Session was devoted to the prevention and management of cardiovascular (CV) risk in patients with inflammatory disorders.
SLE Patients
Ian Bruce, MD, FRCP, University of Manchester, Manchester, UK, presented data that outlined the risk factors for coronary heart disease (CHD) in SLE patients.
SLE patients aged <55 years have been shown to have significantly more carotid plaque (21% vs 3%; p<0.01) compared with control subjects [Ahmad Y et al. Rheumatology 2007]. This may be related to the inflammatory mechanisms that are central to SLE, such as the interferon-1 and complement pathways that appear to be important factors in atherogenesis. In addition, low TGF-β 1 activation that is seen in SLE patients is linked to increased lymphocyte apoptosis, irreversible organ damage, disease duration, calculated low-density lipoprotein levels, and increased carotid intima-media thickness (IMT) and therefore may also aid in the promotion of early atherosclerosis [Jackson M et al. Arthritis Res Ther 2006].
When hypertension and diabetes mellitus, also more prevalent in SLE patients, are accounted for, SLE remains independently associated with an increased risk for CHD. Persistent hypercholesterolemia, found in 34% to 51% of patients with SLE, also appears to be an independent risk factor.
Dr. Bruce discussed measures to reduce CV risk, such as the use of the anti-malarial hydroxychloroquine to treat the pain and swelling of arthritis. He noted that low-dose steroids have a beneficial anti-inflammatory effect, although high doses may be detrimental because they exacerbate metabolic risk factors. Dr. Bruce suggested screening SLE patients for CHD, minimizing both inflammatory disease activity and overall steroid exposure, and using hydroxychloroquine and low-dose aspirin judiciously.
Rheumatoid Arthritis (RA) Patients
Alexandre Voskuyl, MD, PhD, VU University Medical Center, Amsterdam, The Netherlands, presented current data that concern the management of CV complications in RA patients.
RA patients have more than twice the risk for congestive heart failure, ischemic heart disease, myocardial infarction, and peripheral vascular disease compared with the general population. In addition to the classic risk factors (uncontrolled hypertension, dyslipidemia, and diabetes), specific risk factors for CVD-related mortality, morbidity, or subclinical atherosclerosis in RA patients include consistent inflammation, disease duration, higher ESR, extra-articular features, and rheumatoid factor. Joint damage has been shown to be associated with increased IMT, a surrogate marker of CVD.
In patients with RA, disease-modifying antirheumatic drugs (DMARDs), in particular methotrexate, and biologics may reduce CV risk by reducing inflammatory pathways that are important in the development of atherosclerosis and by reducing the effect of other CVD risk factors (eg, improving atherogenic lipid profile, improving physical fitness, and improving insulin resistance).
As a management strategy, Associate Prof. Voskuyl suggests screening RA patients for CVD risk factors, treating hypertension and dyslipidemia according to current guidelines, and using anti-platelet therapy when appropriate. Consideration also should be given to reducing disease activity more profoundly with (change of) DMARDs and biologics.
Systemic Sclerosis (SSc) Patients
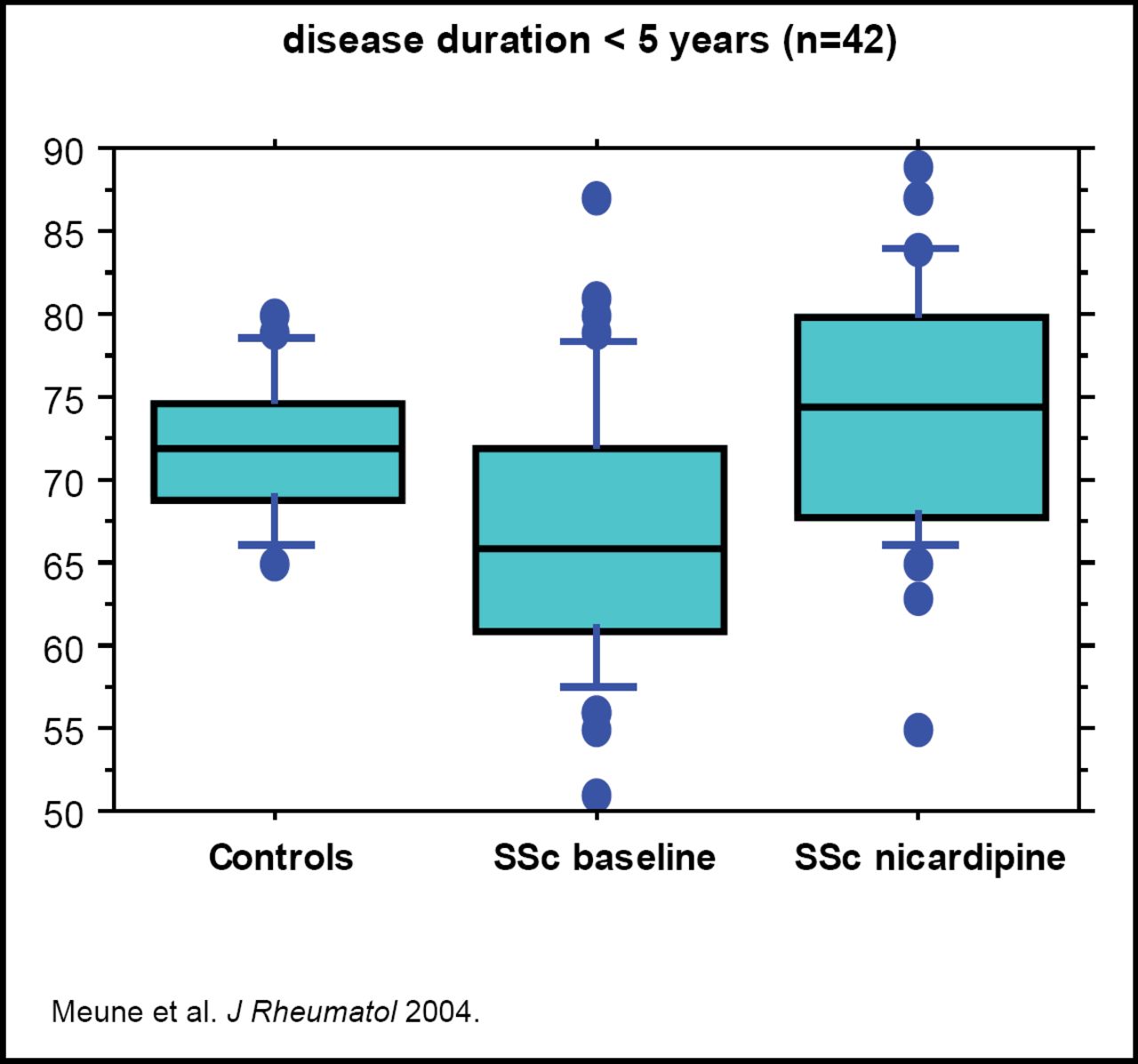
Myocardial involvement due to microcirculation impairment is frequent in the majority of SSc patients. Andre Kahan, MD, Hôpital Cochin, Paris, France, reported on several studies that showed that calcium channel inhibitors (nifedipine and nicardipine), ACE inhibitors (captopril), and the endothelin receptor antagonist bosentan may be useful treatments to improve myocardial perfusion and metabolism, and left and right ventricular functions in SSc patients [Vignaux O et al. Ann Rheum Dis 2005; Allanore Y et al. J Rheumatol 2006; Meune C et al. J Rheumatol 2004] (Figure 1).

Left Ventricular Ejection Fraction in SSc.
RA Resembles Type 2 Diabetes as Risk Factor for CVD
Mike Peters, MD, VU University Medical Center, Amsterdam, The Netherlands, presented data from the CARRÉ study, which compared the prevalence of CVD in RA patients with normal fasting glucose levels with the prevalence of CVD in patients from the Hoorn Study
[Dekker JM et al. Circulation 2005] who had either normal fasting glucose levels or type 2 diabetes. The prevalence of CVD was 9.7% (95% CI, 6.0% to 13.4%) in Hoorn study subjects with normal glucose levels and 21.6% (95% CI, 15.7% to 27.5%) in those with type 2 diabetes versus 15.7% (95% CI, 11.4% to 20.0%) in RA subjects with normal glucose levels. No significant difference in prevalence was observed between RA patients with normal glucose levels and those with type 2 diabetes, suggesting a similar CVD risk in the 2 diseases.
RA is an Important Independent Risk Factor for Incident CVD
In another study that was presented by Prof. Peters, RA was shown to be an independent, significant (p≤0.01) risk factor for CVD compared with the general population. Data from CARRÉ that analyzed the 3-year incidence of CVD in 363 RA patients noted at least 1 CV event in 8.6% of the RA patients versus in 4.3% of the general population, corresponding with an incidence of 3.14/100 patient-years (95% CI, 1.98–4.30) for RA patients and 1.51/100 patient-years (95% CI, 1.18–1.84) for the general population. Even after adjustment for a higher prevalence of traditional CV risk factors that normally are found in RA patients, the CVD risk in patients with RA remains significantly elevated compared with the general population.
CV Risk Among Patients with RA in CORRONA
Daniel Solomon, MD, Brigham and Women's Hospital, Boston, MA, presented data from the CORRONA registry, which contains data on over 14,000 RA patients. The study compared CV risk factors (CVRFs) with RA disease factors (RADFs) with the goal of developing more robust clinical prediction rules for cardiovascular outcomes. CVRFs included a history of coronary artery disease or myocardial infarction (MI), diabetes, hypertension, family history of premature MI, low body mass index (BMI), dyslipidemia (assessed as use of a lipid-lowering agent), race, and current tobacco use. RADFs included duration of RA, RF status, HAQ, clinical disease activity index (CDAI), subcutaneous nodules, Sjögrens, tender joint count, swollen joint count, and total joint replacements. In multivariable Cox regression models, the CVRFs with increased relative risks (RR) included race (RR 1.26), low BMI (RR 1.25), prior MI (RR 1.75), and tobacco use (RR 1.92). The RADFs with increased RRs were subcutaneous nodules (RR 1.44), HAQ-DI (RR 1.20), and the CDAI (RR 1.06). Overall c-statistic was 0.80, suggesting that CVRFs and RADFs share similar explanatory value in explaining CV endpoints.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.