

Summary
When the results of the Investigation of Lipid Level Management Using Coronary Ultrasound to Assess Reduction of Atherosclerosis by CETP Inhibition and HDL Elevation [ILLUSTRATE] trial [Nissen SJ et al. N Engl J Med 2007] called into question the efficacy of the cholesteryl ester transfer protein (CETP) inhibitor torcetrapib, many thought it signaled the end of the pursuit of these compounds for the treatment of dyslipidemia. This article discusses new data from ILLUSTRATE, which provide hope for the future of CETP inhibitors.
- lipid disorders
When the results of the ILLUSTRATE (Investigation of Lipid Level Management Using Coronary Ultrasound to Assess Reduction of Atherosclerosis by CETP Inhibition and HDL Elevation) trial [Nissen SJ et al. N Engl J Med 2007] called into question the efficacy of the cholesteryl ester transfer protein (CETP) inhibitor torcetrapib, many thought it signaled the end of the pursuit of these compounds for the treatment of dyslipidemia. Steven E. Nissen, MD, Cleveland Clinic, OH, discussed new data from ILLUSTRATE, which provide hope for the future of CETP inhibitors.
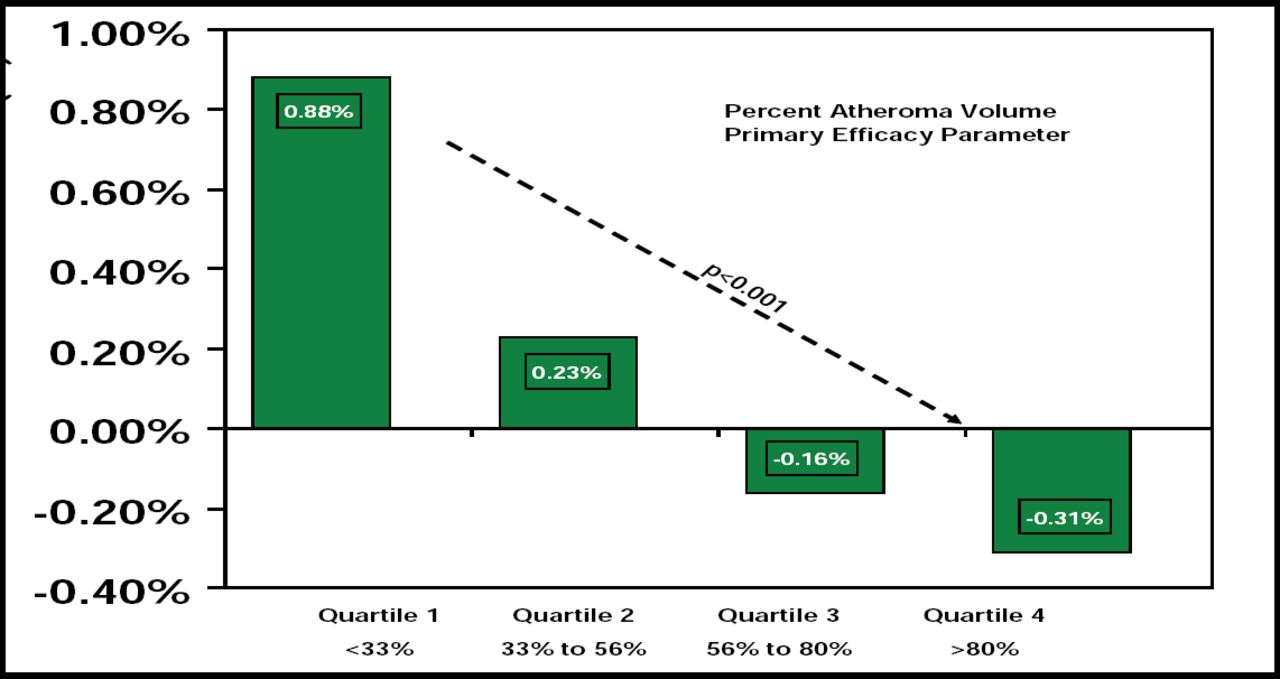
Although ILLUSTRATE showed that the CETP inhibitor torcetrapib increased HDL-C levels, the primary analysis did not show an effect on atherosclerotic progression. A new secondary analysis of the ILLUSTRATE data has shown that when percentages of HDL-C elevation are viewed as incremental quartiles, there is a progressive decrease in rate of progression of coronary atherosclerosis relative to the extent of HDL-C elevation. Patients who reached the highest HDL-C level (>86 mg/dL) actually achieved atherosclerosis regression (Figure 1).

Torcetrapib Results: Quartiles of HDL-C Elevation.
Several new CETP inhibitors are entering clinical trials, and Dr. Nissen expressed hope that the newer drugs might prove to be clinically useful, because they do not appear to cause an increase in blood pressure, as was shown with torcetrapib.
Johan W. Jukema, MD, Leiden University Medical Center, Amsterdam, The Netherlands, spoke about statin therapy in three subgroups of patients who are known to be at risk for cardiovascular (CV) events: patients with chronic kidney disease, older patients with moderate to severe ischemic systolic heart failure, and the at-risk elderly.
According to Prof. Jukema, study results are mixed for the first two groups. For patients with chronic kidney disease, he cited results from a meta-analysis that showed that the use of statins can significantly reduce lipid concentrations (total cholesterol −42.28 [95% CI, −47.25 to −37.32]; LDL-C −43.12 [95% CI, −47.85 to −38.40]; HDL-C +0.41 [95% CI, −0.78 to 1.60]; and triglycerides −23.71 [95% CI, −33.52 to −13.90]), as well as mortality (RR 0.81; 95% CI, 0.73 to 0.90), but that they provide no benefit for all-cause mortality (RR 0.92, 95% CI, 0.82 to 1.03) [Strippoli GFM et al. Br Med J 2008].
For older patients with ischemic systolic heart failure, Prof. Jukema cited new data from CORONA (Controlled Rosuvastatin Multinational Trial in Heart Failure), which showed that although the use of rosuvastatin 10 mg daily significantly decreased the number of related hospitalizations (2564 vs 2193, placebo vs rosuvastatin, respectively; p<0.001), there was no effect on the primary composite endpoint of death, non-fatal MI, or non-fatal stroke (HR 0.92; 95% CI, 0.83 to 1.02; p=0.12) [Kjekshus J et al. N Engl J Med 2007]. These findings were surprising because prior retrospective analyses with atorvastatin 80 mg [Scirica BM et al. J Am Col Cardiol 2006; Khush KK et al. Circulation 2007] had suggested that such patients might benefit from high-dose statin therapy.
Prof. Jukema also discussed the results of a meta-analysis that examined the effect of statin therapy for secondary prevention in elderly patients with coronary heart disease, which showed that not only do statins reduce all-cause mortality in these patients (15.6% with statins vs 18.7% with placebo, RR reduction 22% over 5 years; 95% CI, 0.65 to 0.89), but the extent of the effect is much larger than originally thought [Afilalo J et al. J Am Col Cardiol 2008; Table 1].
Effect of Statin Therapy for Secondary Prevention in the Elderly.
Robert S. Rosenson, MD, University of Michigan, Ann Arbor, MI, reviewed several studies that evaluated the relationship between obesity and mortality, noting that while obese individuals (BMI 30–35) may not have an increased risk for mortality (RR 0.97; 95% CI, 0.82–1.15), the risk is increased for the severely (BMI >35) obese (RR 1.88; 95% CI, 1.05–3.34) [Romero-Corral A et al. Lancet 2006].
Investigators who evaluated the differences in risk among obese and severely obese individuals have suggested that insulin sensitivity may be a better predictor than obesity alone in predicting risk (Table 2; McLaughlin T et al. Arch Int Med 2007; Reaven G. Diab Vasc Dis Res 2005).
CV and Diabetes Risk Factors in Obese Individuals Based on Tertile of SSPG Concentration.
Dr. Rosenson noted that cardiovascular risk is heterogeneous among obese individuals and that more emphasis should be placed on identifying individuals at risk for cardiovascular disease based on their level of insulin resistance versus obesity alone.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.