

Summary
This article provides an overview of cardiac resynchronization therapy (CRT) in patients with atrial fibrillation (AF), including the effect of AF on CRT outcomes and strategies for CRT pacing in AF patients.
- heart failure
- interventional techniques & devices
- arrhythmias
CRT in AF
Michael R. Gold, MD, Medical University of South Carolina, Charleston, SC, provided an overview of cardiac resynchronization therapy (CRT) in patients with atrial fibrillation (AF), including the effect of AF on CRT outcomes and strategies for CRT pacing in AF patients.
AF is frequent in patients with congestive heart failure (CHF) and reduces the efficacy of CRT in several ways. Biventricular pacing is less frequent in the presence of AF, irregularities of the ventricular response adversely affect the filling and emptying of the left ventricle, and the presence of AF leads to the inability to optimize atrioventricular timing to maximize contractility and preload.
AF is the most common arrhythmic cause of hospitalization for patients on CRT. Data from a prospectively collected registry of patients from February 1999 to October 2005 who had CRT devices implanted showed that hospital stays for patients with AF were twice as long as those for patients without AF. In addition, ICU admissions were 3 times as frequent (41% vs 14%), and the use of ionotropic therapy increased by about 50% [Kahn et al. HRS 2006].
Despite these effects, data from the CARE-HF study have shown that CRT reduces mortality regardless of whether patients developed AF [Hoppe UC et al. Circulation 2006]. Pacing strategies for patients with AF include aggressive rhythm and rate control with antiarrhythmic therapy and increasing the lower rate of pacing to maintain a higher biventricular pacing rate. Other features and devices that can be used to maintain the percentage of ventricular pacing include ventricular r ate regulation, triggered pacing modes, and AV node ablation.
Mechanisms Associated with CRT Benefit
We know that 20–30% of patients respond to CRT [Bax J et al. J Am Col Cardiol 2005]. Jeroen J. Bax, MD, University Hospital Leiden, Leiden, The Netherlands, provided some insight into why this might be so and whether QRS is an appropriate predictor of CRT response.
Although it is not clear what exactly drives the benefit of CRT, most studies indicate that it is LV dyssynchrony [Bax J et al. J Am Col Cardiol 2005]. However, when Bleeker and colleagues studied 90 patients with end-stage heart failure (HF) and QRS ranging from 80 to 240, they found no correlation between QRS duration and left ventricular (LV) dyssynchrony (r=0.26; p=NS) [Bleeker GB. J Cardiovasc Electrophysiol 2004].
Further, when patients were stratified by duration of QRS interval, 30% to 40% of HF patients with QRS >120 ms did not exhibit LV dyssynchrony, which may explain the lack of response of some patients to CRT.
Alternatively, 27% of patients with HF and a narrow QRS complex show significant LV dyssynchrony and may be candidates for CRT. Thus, if response to CRT is related to LV dyssynchrony, then QRS duration may not be all that important in determining the response to CRT. In Prof. Bax's view, larger studies are needed to help answer these questions.
Duration of Benefit Associated with CRT
William T. Abraham, MD, Ohio State University, Columbus, OH, discussed the benefits that are seen with CRT and whether these results can be sustained.
More than 4000 NYHA Class III or IV patients on CRT have been evaluated in randomized controlled trials. The short term results of these trials (usual duration, 6 months) have demonstrated consistent improvement in quality of life (QOL) (significant improvement on the Minnesota Living with Heart Failure Score), functional status improvement (≥1 improvement in NYHA class), and exercise capacity (improvements in 6 minute walk distance or peak VO2). The trials also have provided strong evidence for reverse remodeling—eg, lower LV volumes and dimensions, higher LVEF, and lower mitral regurgitation, as well as a reduction in HF and trends toward reductions in all-cause morbidity and mortality [Abraham WT & Hayes DL. Circulation 2003].
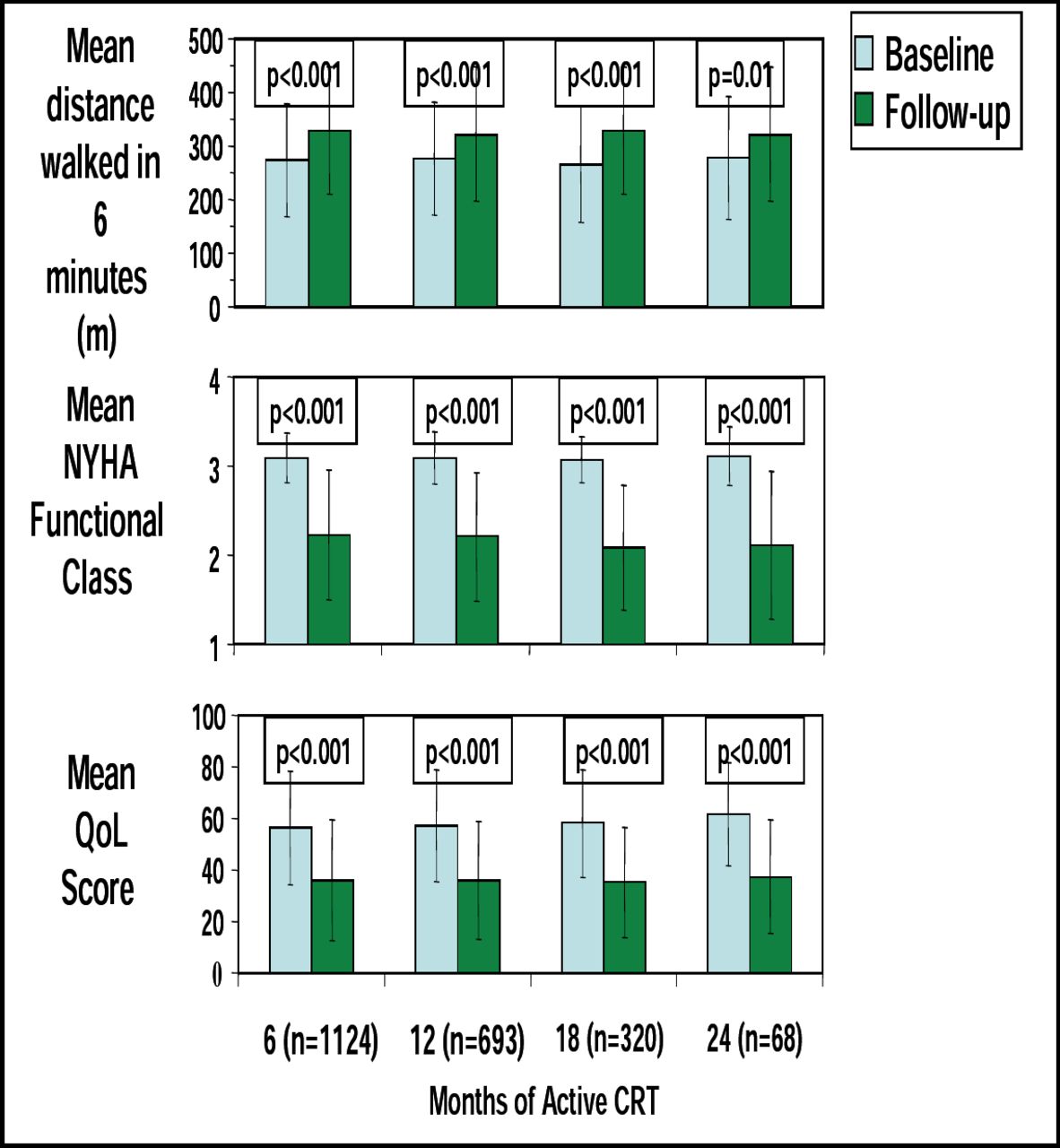
One of the questions that must be answered, however, is “Are these results sustained?” According to data from the MIRACLE trial, the improvement in QOL scores, 6 minute walk distance, and NYHA Functional class appear to be sustained out to at least 24 months (Figure 1) [Abraham WT. AHA 2003]. In terms of outcomes and remodeling, the CARE-HF Extension study demonstrated a 40% reduction in all-cause mortality associated with CRT after a mean follow-up of 36.4 months (p<0.0001). Significant improvements were also seen in time to death from worsening HF (45%; p=0.003) and time to sudden cardiac death (46%; p=0.006).

CRT Benefits Sustained Through 2 (Years Paired Data Displayed).
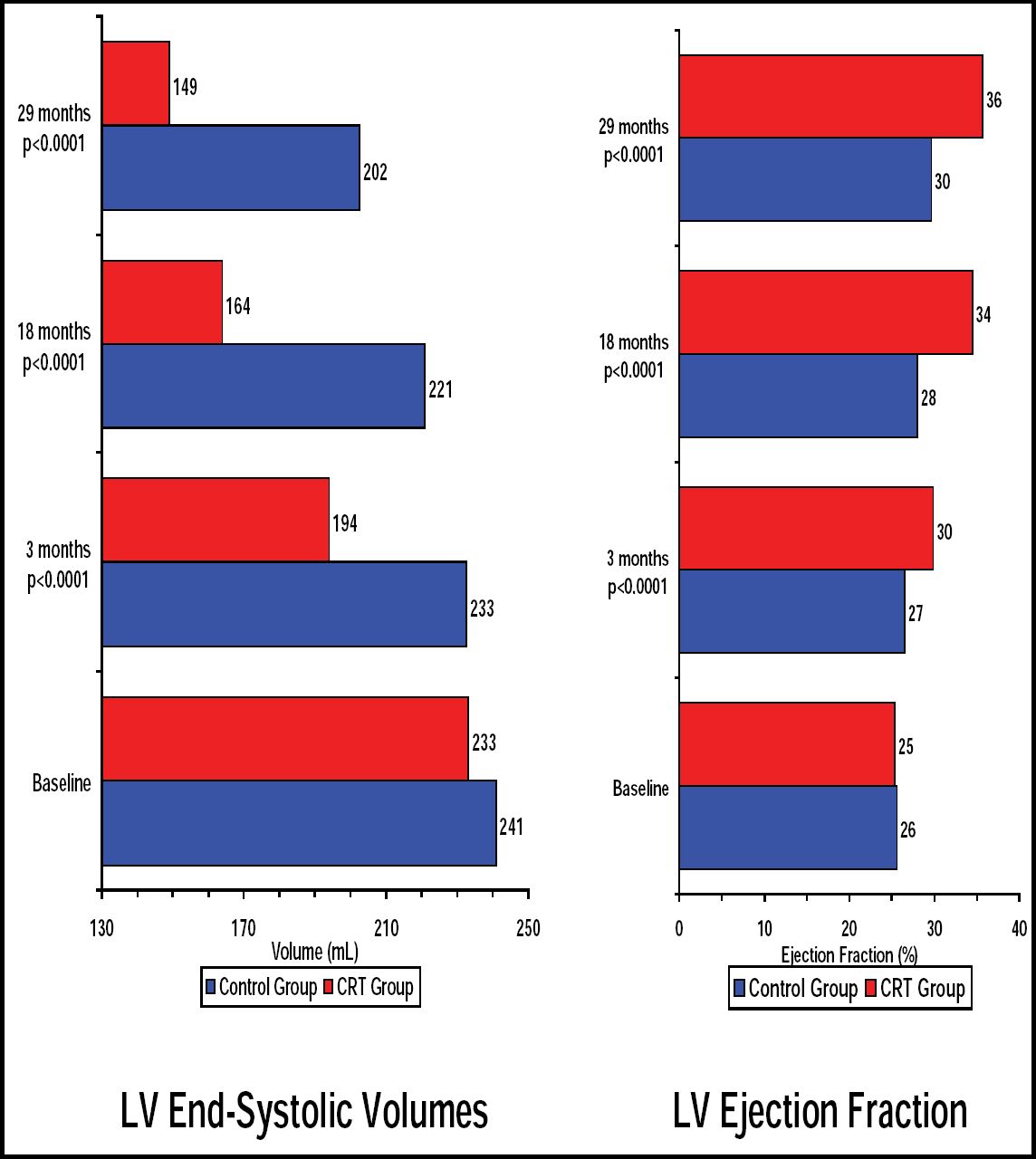
According to Dr. Abraham, remodeling is probably our best surrogate for the efficacy of HF therapy. The initial improvements in both LV end systolic volume (LVESV) and LVEF observed with CRT in the CARE HF trial were sustained through 29 months (Figure 2). What is most interesting about reverse remodeling observed to date with CRT is that it appears to be progressive over a long period of time, implying that the improvements with CRT are sustainable.

CARE-HF: Changes in LVESV and LVEF.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.