

Summary
Recent controversy has surrounded the discovery of a small but definite increase in late stent thrombosis with drug-eluting stents (DES). Despite the increased risk for late stent thrombosis with DES, these stents may be preferable to bare metal stents in certain patient subgroups. This article discusses best practices when selecting patients for DES.
- interventional techniques & devices
- thrombotic disorders
Recent controversy has surrounded the discovery of a small but definite increase in late stent thrombosis with drug-eluting stents (DES), explained Philippe Gabriel Steg, MD, Hôpital Bichat, Paris, France. Despite the increased risk for late stent thrombosis with DES, these stents may be preferable to bare metal stents (BMS) in certain patient subgroups. In this plenary session, Professor Steg shared his approach to selecting patients for DES.
Long-Term Outcomes with DES
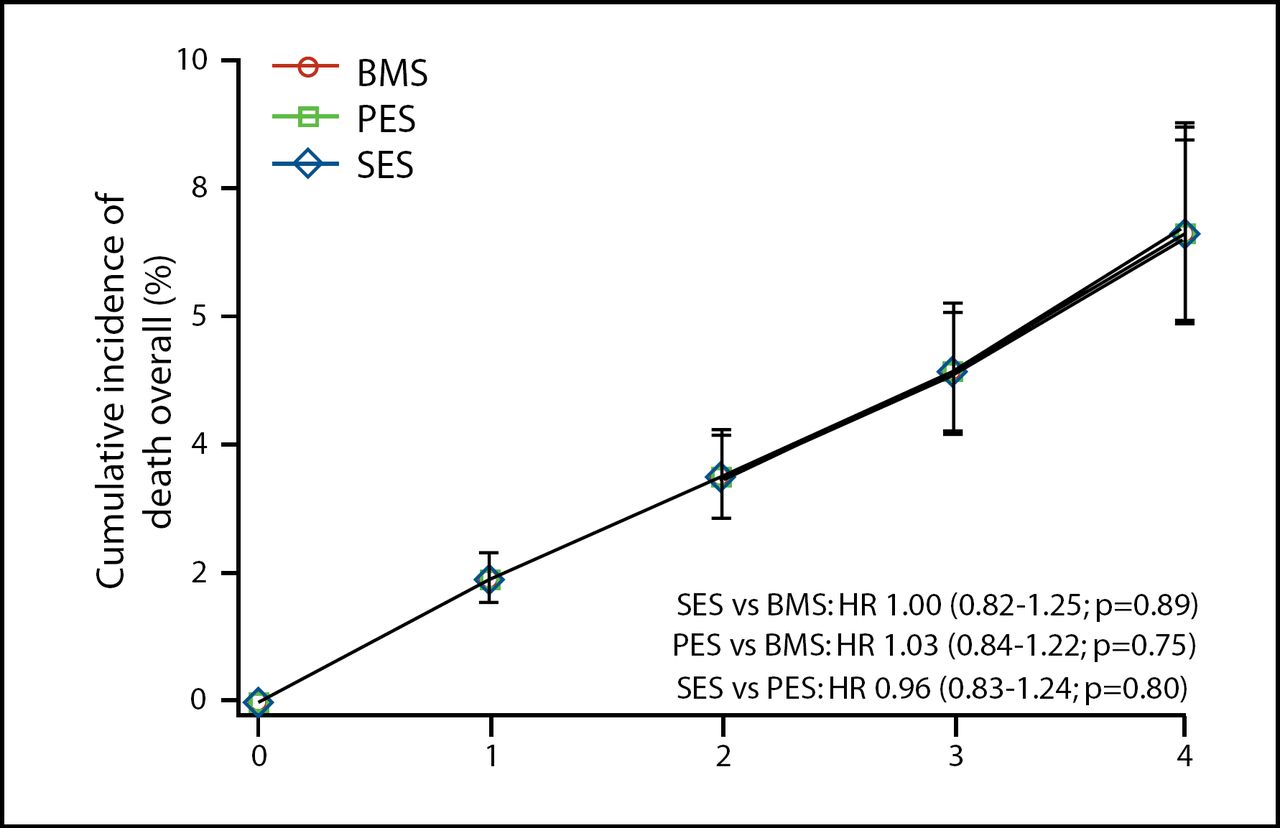
To date, there is no randomized clinical trial evidence linking DES with worse long-term clinical outcomes, Professor Steg said. In a comprehensive meta-analysis of 39 randomized clinical trials (n=18,023), the 4-year mortality estimates following BMS and DES, including sirolimus-eluting stents (SES) and paclitaxel-eluting stents (PES), were nearly identical (Figure 1) [Stettler C et al. Lancet 2007].
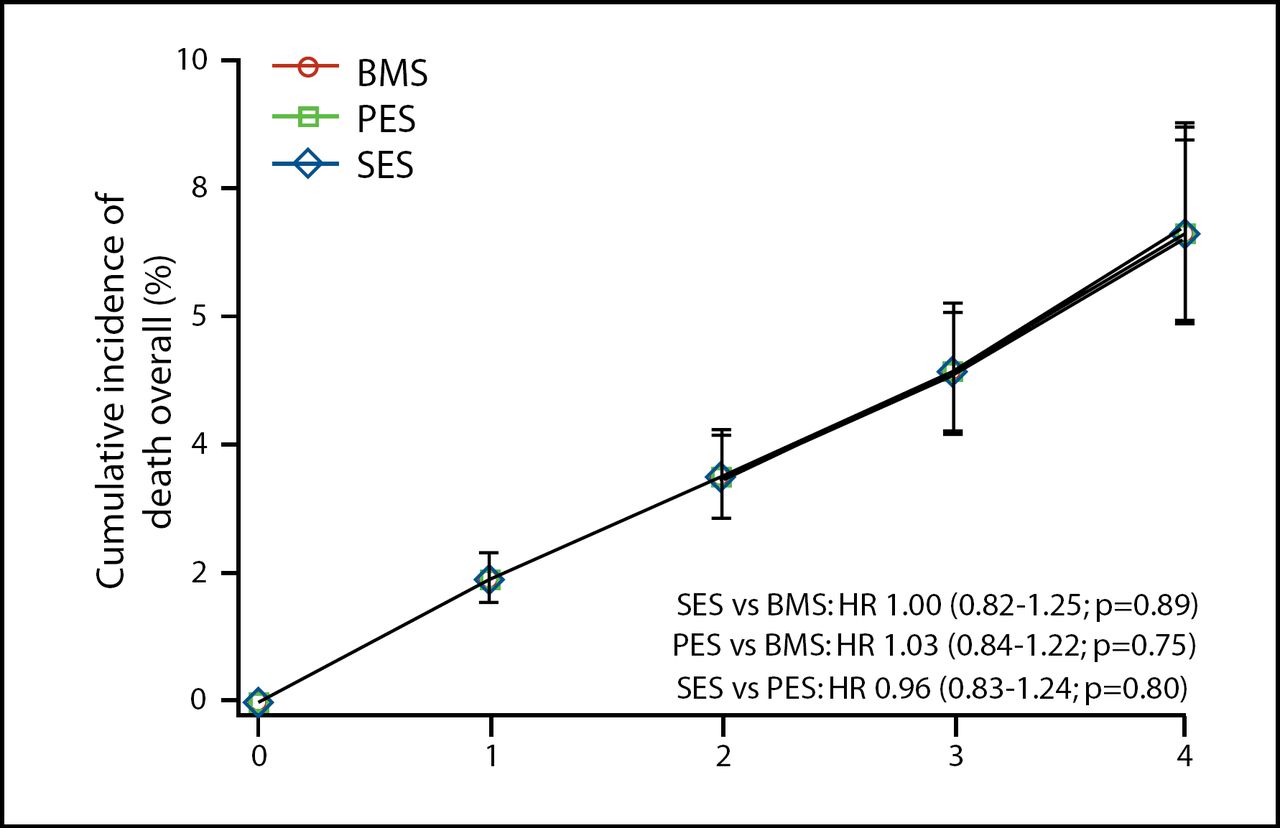
Four-Year Mortality with Bare Metal and Drug-Eluting Stents.
BMS=bare metal stent, PES=paclitaxel-eluting stent, SES=sirolimus-eluting stent
Reprinted from The Lancet, Vol 370, Settler C et al, 937–948, copyright 2007, with permission from Elsevier.
Data from large registries have provided conflicting views about the long-term clinical outcomes associated with DES. For example, in the Swedish Coronary Angiography and Angioplasty Registry (SCAAR), there was a trend toward a lower event rate in the DES group (n=6,033) compared with the BMS (n=13,738) group (RR 0.94, 0.83–1.06) within the first 6 months of stent implantation. However, from 6 months to 3 years, the risk of death or MI was greater for patients who received DES (RR 1.20, 1.05–1.37) [Lagerqvist B et al. N Engl J Med 2007].
In contrast to SCAAR data, 2-year outcomes in the Massachusetts stent (MASS Stent) registry favored the use of DES (n=11,516) compared with BMS (n=6,210). Two years following the index intervention, patients in the DES group had a significantly lower risk of mortality (9.4% vs 11.9% for BMS; p<0.0001) and revascularization (20.1% vs 23.9%; p<0.0001). There was also a trend toward lower MI risk among patients who received DES compared with BMS recipients (10.8% vs 11.8%; p=0.11) [Mauri L et al. American Heart Association 2007].
Long-Term Dual Antiplatelet Therapy After Stenting
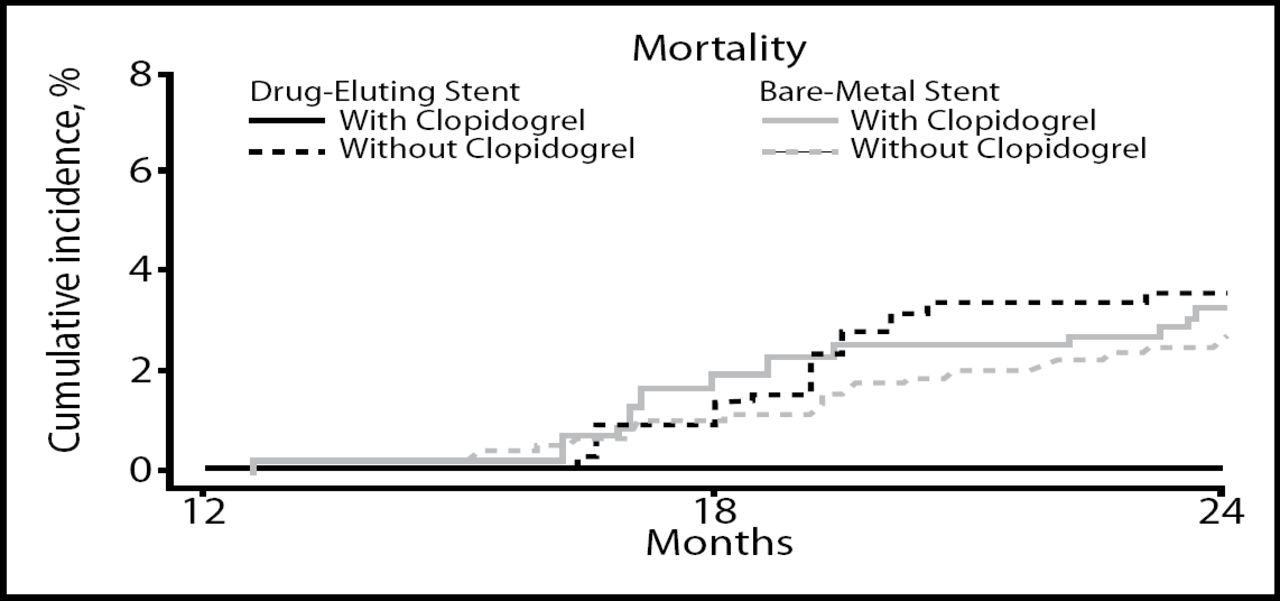
According to an observational study at the Duke Heart Center, early discontinuation of clopidogrel following stent implantation increases the risk of death and MI. Compared with patients who discontinued clopidogrel therapy within the first 12 months, those who remained on clopidogrel had a lower risk of death (3.5% vs 0%; p=0.004; Figure 2) or the combined endpoint of death or MI (4.5% vs 0%; p<0.001) at 24 months [Eisenstein EL et al. JAMA 2007]. These findings suggest that stent placement requires at least 1 year of antiplatelet therapy, Professor Steg said.
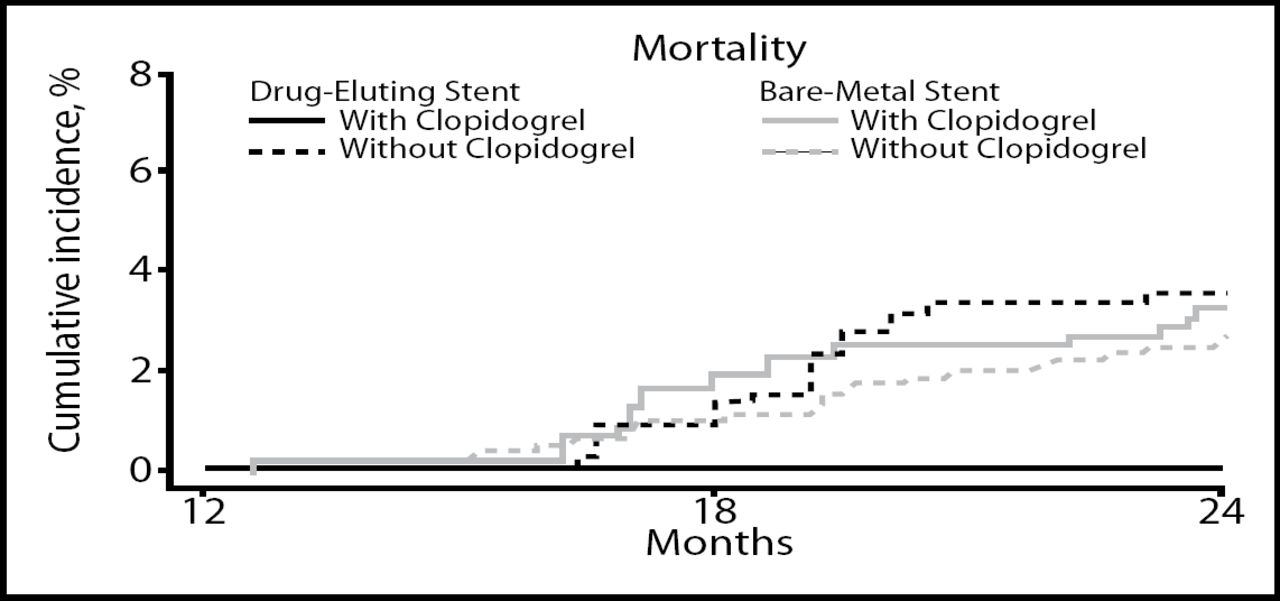
Mortality Based on Clopidogrel Use at 12 Months.
“If early discontinuation is associated with catastrophic outcomes, then DES should only be placed in patients who are able to comply with and tolerate long-term dual antiplatelet therapy,” Professor Steg said. He advised that DES should not be placed in patients who:
-
have a history of ongoing bleeding
-
have a high risk of bleeding
-
may not be compliant to long-term dual antiplatelet therapy
-
may require early discontinuation of antiplatelet therapy because of scheduled procedures, such as planned surgery
-
require long-term oral anticoagulants
Role of Restenosis Risk
Important risk factors for restenosis were recently identified in the Cardiac Care Network of Ontario (CCNO) registry (n=13,353). In this population of patients undergoing PCI, the three strongest risk factors for restenosis included diabetes, small vessels (<3 mm in diameter), and long lesions (>20 mm) [Tu JV et al. NEJM 2007].
Although the majority of stented patients in the CCNO registry was at low risk for target vessel revascularization, DES was associated with a lower rate of revascularization than BMS at 2 years (7.4% vs 10.7%; p<0.001). Among the highest-risk patients – those with all three restenosis risk factors – the benefit of DES was more dramatic. In this group, the rate of target vessel revascularization at 2 years was 7.2% for DES and 17.6% for BMS (HR 0.38; p<0.001) [Tu JV et al. NEJM 2007].
Given evidence that DES is more effective than BMS in preventing restenosis and reducing the need for target vessel revascularization, DES should be the preferred stent in high-risk patients, Professor Steg said.
Role of Diabetes
Patients with diabetes, who often have multivessel disease with long lesions in small vessels, appear to be particularly good candidates for DES, Professor Steg said. However, the optimal type of stent for this patient group has recently been questioned.
Worse outcomes with DES in diabetic patients were reported in a meta-analysis of four trials comparing SES and BMS. In the overall study population (n=1,748), 4-year survival was similar in the SES and BMS groups (93.3% vs 94.6%; p=0.28). However, in the subgroup of patients with diabetes (n=428), survival was significantly lower in the SES group (87.8% vs 95.6% in the BMS group). The hazard ratio for death among diabetics in the SES group was 2.9 (95% CI, 1.38–6.10; p=0.008) [Spaulding C et al. NEJM 2007].
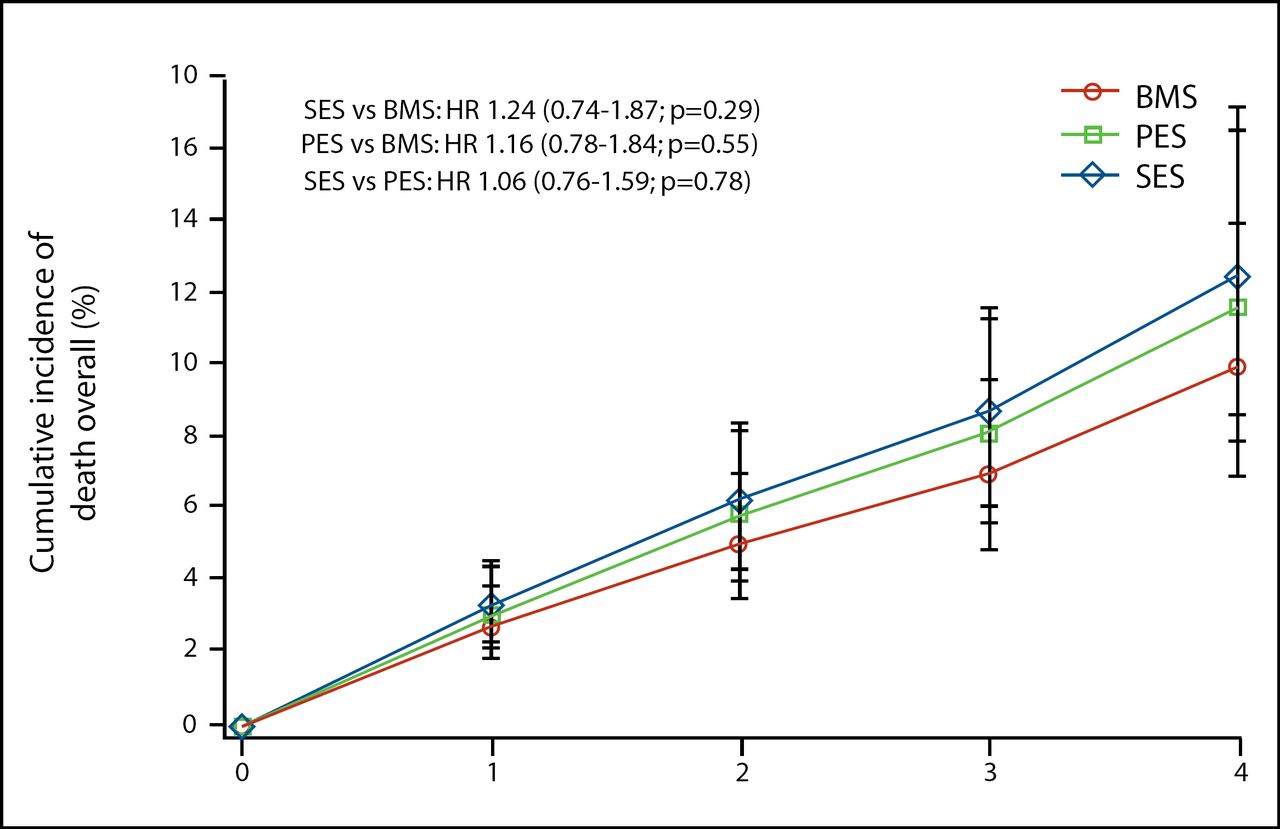
In contrast to these findings, results of a 39-trial meta-analysis suggested that the presence of diabetes does not increase the risk of death or MI among patients receiving DES. In the subgroup of patients with diabetes (n=3,762), the risk of death was not significantly higher for SES versus BMS (HR 1.24, 0.74–1.87; p=0.29), nor for PES versus BMS (HR 1.16, 0.78–1.84; p=0.55; Figure 3). Risk for the combined endpoint of death or MI was not significantly elevated in diabetic patients who received SES (HR 1.03, 0.79–1.35; p=0.87) or PES (HR 1.08, 0.79–1.43; p=0.62) compared with BMS [Stettler C et al. Lancet 2007].
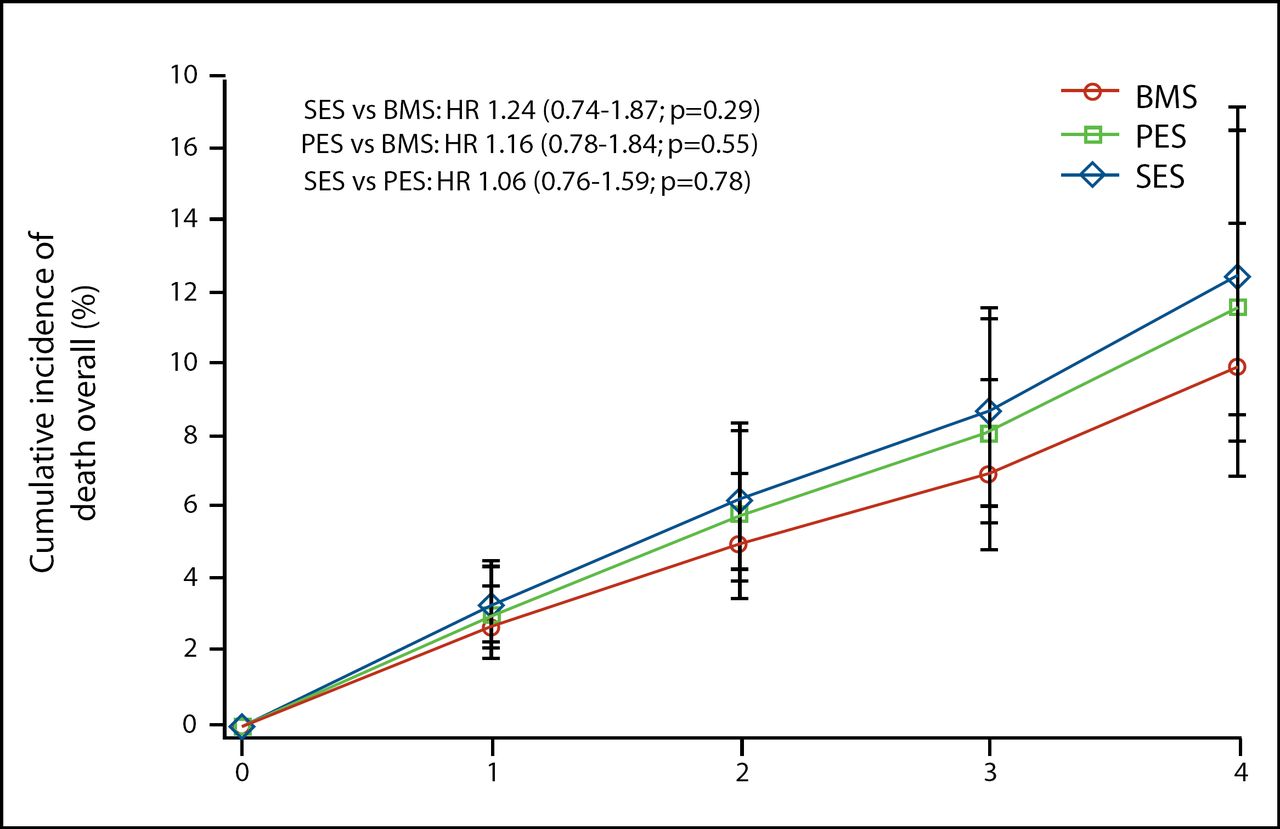
Four-Year Mortality in Patients with Diabetes.
BMS=bare metal stent, PES=paclitaxel-eluting stent, SES=sirolimus-eluting stent
Reprinted from The Lancet, Vol 370, Settler C et al, 937–948, copyright 2007, with permission from Elsevier.
As an alternative to stent implantation, “coronary artery bypass surgery (CABG) is an extraordinarily effective option for treating and revascularizing multivessel disease in patients with diabetes,” Professor Steg said.
In the Bypass Angioplasty Revascularization Investigation (BARI) trial, 1,829 patients with multivessel disease were randomly assigned to intervention with percutaneous transluminal coronary balloon angioplasty (PTCA) or CABG. Whereas 10-year survival was similar for PTCA (71.0%) and CABG (73.5%) in the overall study population, CABG showed a significant survival advantage among patients with diabetes. In these patients, 10-year survival in the CABG and PTCA groups was 57.8% and 45.5%, respectively (p=0.025) [BARI Investigators. JACC 2007].
Conclusion
“Based on current data, we need to have a high probability of restenosis [without DES] and a high probability for long-term compliance and tolerance to dual antiplatelet therapy,” to increase the likelihood of long-term success with DES, Professor Steg concluded. He also emphasized the importance of optimal stent placement, which is a critical factor in lowering the risk of late stent thrombosis.
Professor Steg cautioned that routine use of DES may be premature for diabetic patients with diffuse lesions, for primary PCI in patients with STEMI, or for untested indications. Results of large randomized clinical trials with long-term follow-up are awaited in some of these indications, he said.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.