

Summary
Imagine a world where there was equality in health care. Imagine that access to a doctor and treatment was unrelated to race, skin color, native country, employment, or the social circumstance into which one was born. This is the world Sir Michael Marmot, FRCP, University College, London, United Kingdom, asked Scientific Sessions 2007 attendees to work toward, in the Lewis A. Conner Memorial Lecture.
- affordability of care
- prevention & screening
“Rise up with me against the organization of misery.” ∼Pablo Neruda
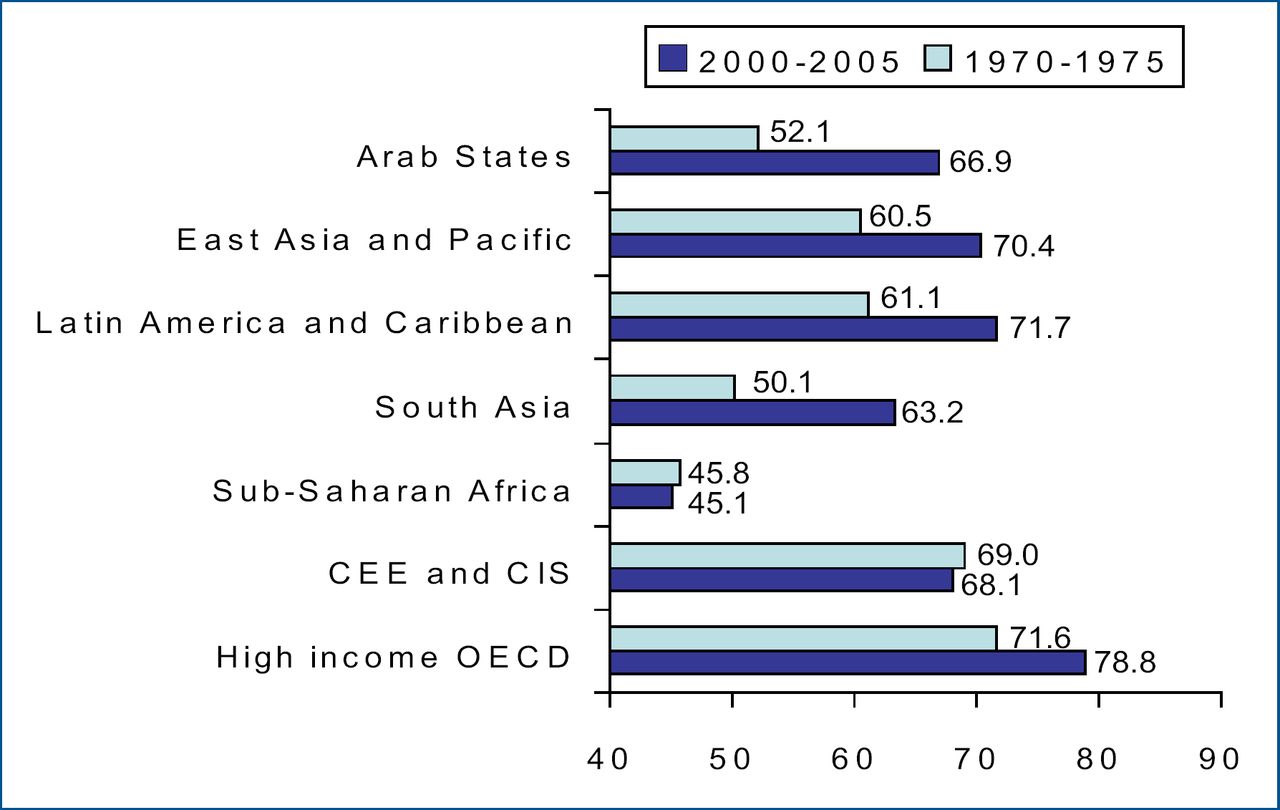
Imagine a world where there was equality in health care. Imagine that access to a doctor and treatment was unrelated to race, skin color, native country, employment, or the social circumstance into which one was born. This is the world Sir Michael Marmot, FRCP, University College, London, United Kingdom, asked Scientific Sessions attendees to work toward, in the Lewis A. Conner Memorial Lecture. “The issue of disparity in health, or as we call them inequalities or inequities of health, is one of key concern, and it is one that an audience such as this will find central to their activities,” said Dr. Marmot. Such inequalities arise not only from inadequate processes but also social situations, education, and employment. That the level of education of people is related to their mortality has previously been demonstrated. “[Health inequity] is a gradient that runs across the whole of society,” and is not solely a problem of poverty. This difference is evident even within a single country. For example, in Glasgow, Scotland, “deprived” social classes have a life expectancy of 54 years, whereas more affluent people can live to be 82. Such inequalities are not inevitable—changes in life expectancy occur over time; therefore they can be changed. Some countries see improvement over time, while others may experience decline (Figure 1).
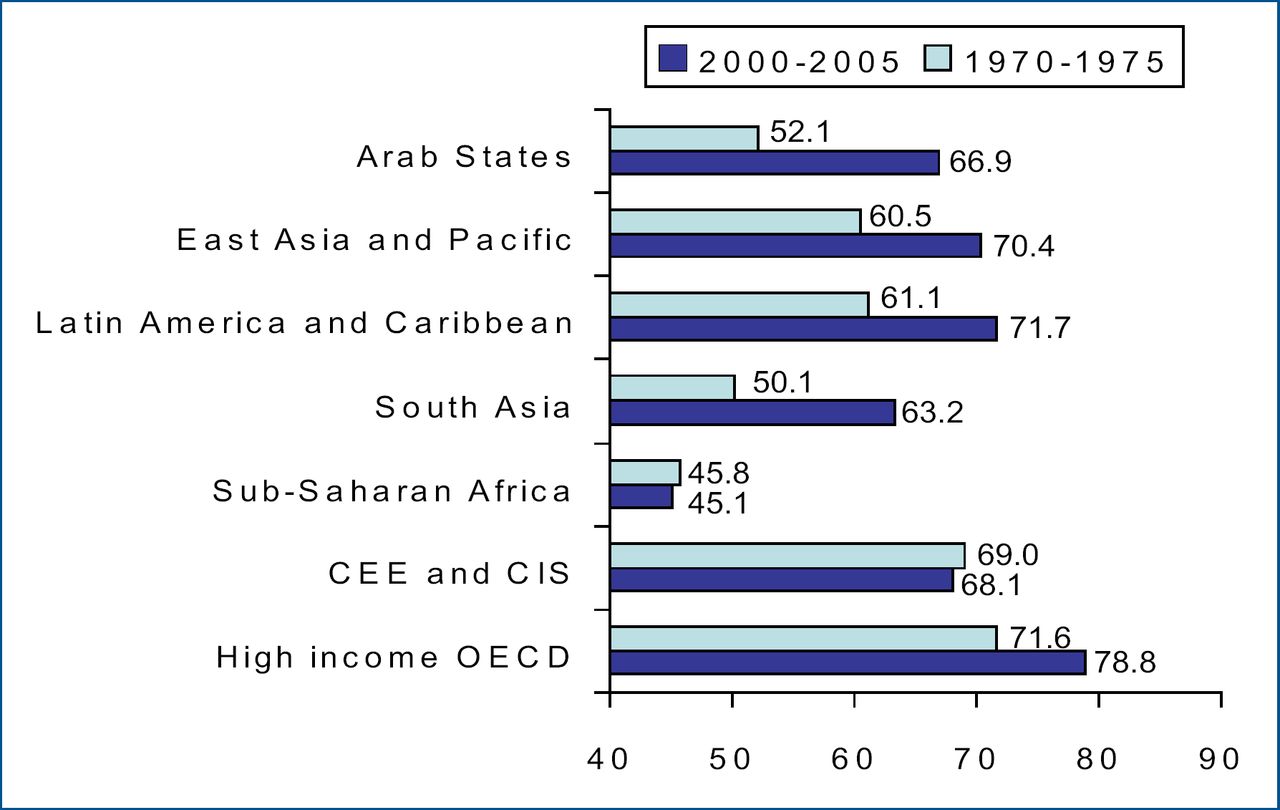
Trends in Life Expectancy – Regions.
Sir Marmot has been involved in the large Whitehall epidemiological studies of British civil servants for over 30 years, which have yielded important insights regarding improved health and life expectancy. One of the key messages is that it is not just money and health insurance that drive the equation. “We need to look at poverty in a different way; it's not simply poverty of material conditions, and it's not simply low income. Indeed, among richer countries, income shows very little relationship to life expectancy,” said Dr. Marmot.
He gave as an example a recent study that evaluated the relative health of residents in the United States compared with a similar sample in the United Kingdom. Data were extracted from large epidemiological surveys in both countries—the US Health and Retirement Survey and National Health and Nutrition Examination Survey in the US, and the English Longitudinal Study of Aging and Health Survey for the UK. The US spends nearly double per capita what is spent on health care in the UK. However, the results of this study indicate that Americans are by and large less healthy than their UK counterparts, as illustrated in the table below:
These findings were consistent in both self-reported and biological measures. Additionally, 94% of Americans in this sample had health insurance coverage; yet they had higher rates of chronic illness such as cardiovascular disease, obesity, and cancer. “As important as health care is, it's not the whole story,” commented Sir Marmot. In terms of the probability of living to age 65, the US ranks 33rd in the world for men, and 36th in the world for women (United Nations Development Program 2005), despite spending 15% of the gross domestic product on health care. “Why don't you drop everything else and ask why are Americans so unhealthy despite the phenomenal amount that you spend on health care?” asked Sir Marmot.
Traditional risk factors such as smoking, drinking, and obesity did not account for the great health differences between the US and the UK, indicating that other factors are involved. The circumstances in which people live and work may hold the key. Job strain, defined as a combination of highly stressful work with a lack of job control, was found to be significantly associated with cardiovascular disease in the Whitehall II study (Kivimaki et al. Am J Hypertens 2007). De Vogli et al (J Epidemiol Community Health 2007) also found a strong relationship between unfairness in the workplace and the incidence of cardiovascular events (hazard ratio 1.55, 95% CI 1.11–2.17) and poor physical (odds ratio 1.46, 95% CI 1.20–1.77) and mental (odds ratio 1.54, 95% CI 1.19–1.99) health in the Whitehall II survey. “We think that people having control over their own lives is vital,” emphasized Sir Marmot.
Sir Marmot currently chairs a World Health Organization commission on social determinants. He told of a successful example of giving people living in poverty more control over their own jobs and lives, leading to better health outcomes. The organization is called the Self-Employed Women's Association (SEWA), which was established in Gujarat, India, to help the 600,000 marginalized women in India who sell vegetables. Through this organization, women have received microcredit, childcare, health care, and the removal of barriers to fair business practices. The SEWA program has been so successful, that they are now focusing on pensions for the participants. “We work under the assumption that health care is central to our lives, that health is a value that everyone has. Health equity is a matter of social justice. If there are inequalities in health care that could be put right if we took appropriate action, then it is unfair and unjust that we do not do it,” concluded Sir Marmot.
For more information visit www.sewa.org
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.