

Summary
This article discusses strategies for long-term antithrombotic therapy, ways to balance the risks and benefits of antithrombotic therapy, as well as gives an overview of evidence supporting the use of long-term antithrombotic therapy after acute coronary syndrome, and suggests strategies for balancing the benefits and risks of long-term antithrombotic therapy for patients with NSTEMI or STEMI.
- thrombotic disorders
- myocardial infarction
Strategies for Long-Term Antithrombotic Therapy
Aspirin therapy has consistently been shown to reduce the rate of cardiovascular events in secondary prevention following a cardiovascular event. However, aspirin alone is not sufficient to prevent ischemic events in patients at high risk, said Freek Verheugt, MD, PhD, Radboud University Nijmegen, The Netherlands. Prof. Verheugt provided an overview of evidence supporting the use of long-term antithrombotic therapy after acute coronary syndrome (ACS).
Dual antiplatelet therapy with clopidogrel and aspirin reduces ischemic events in patients with unstable angina, non-ST-segment elevation myocardial infarction (NSTEMI), or ST-segment elevation MI (STEMI), as well as those undergoing percutaneous coronary intervention (PCI) and stenting [Bhatt DL et al. NEJM 2006; Mehta SR et al. Lancet 2001]. However, long-term treatment with clopidogrel is not necessarily appropriate in a broad population of patients at high risk for cardiovascular events. In the CHARISMA trial, the addition of clopidogrel to aspirin did not appear to reduce the combined risk of MI, stroke, or CV death compared with placebo in patients with multiple risk factors but no established disease (ie, primary prevention cohort) [Yusuf S et al. NEJM 2001].
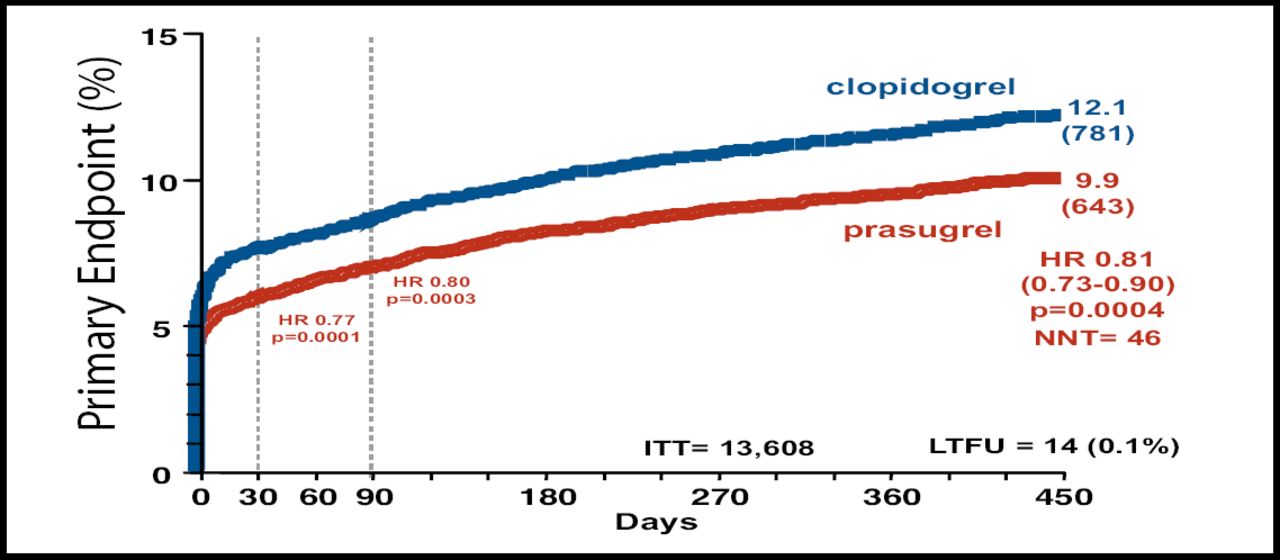
A new generation of antiplatelet agents are currently under evaluation. For example, prasugrel provides more rapid, potent, and consistent inhibition of platelet function than clopidogrel. Compared with clopidogrel, prasugrel reduced the risk of CV death, MI, and stroke by 19% (p=0.0004) and reduced the risk of stent thrombosis by 52% (p<0.0001) in the TRITON-TIMI 38 trial. However, these gains came at the cost of excess major bleeding, including fatal bleeding (HR 1.32; p=0.03; Figure 1) [Wiviott DS et al. NEJM 2007].
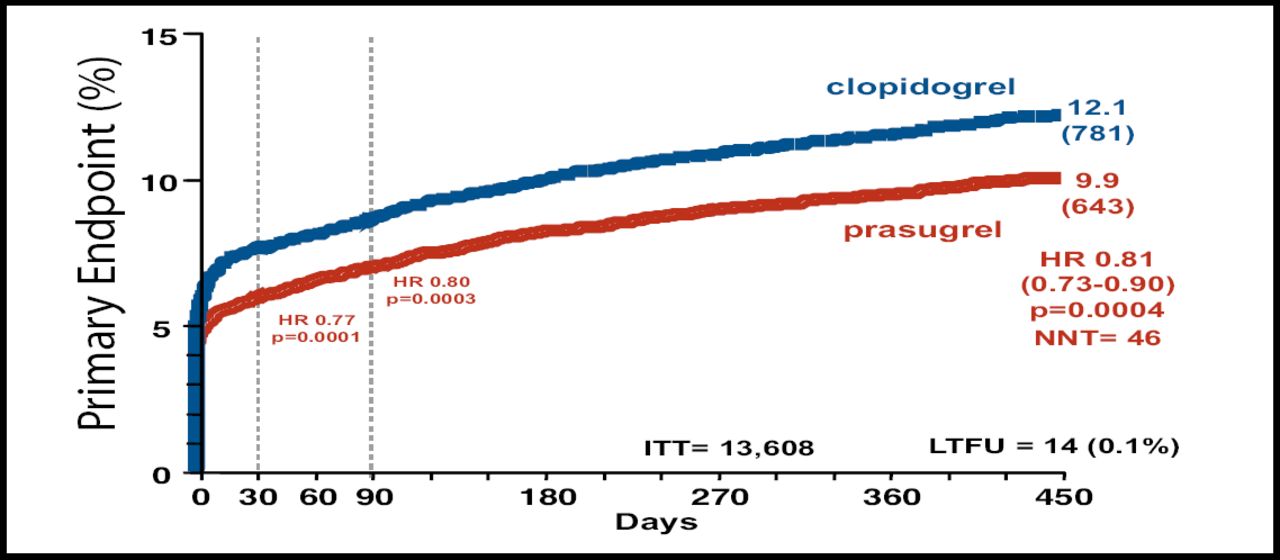
Efficacy and Safety of Prasugrel vs Clopidogrel in Patients Scheduled for PCI. Primary efficacy endpoint: CV death, MI, and Stroke. Safety Endpoint: TIMI Major Bleeding.
Prof. Verheugt summarized his presentation by discussing the ideal duration of different therapies for different patient types. For example, he recommended the use of low-dose aspirin (<100 mg) for all patients, adding that the optimal duration of treatment is “forever”.
Prof. Verheugt advised that clopidogrel may be appropriate for 1 year in patients with NSTEMI who were treated with or without PCI, and for STEMI patients who were treated with PCI. For STEMI patients who did not undergo PCI, clopidogrel may be beneficial for approximately 1 month. For both NSTEMI and STEMI patients who were treated with drug-eluting stents, the optimal duration of clopidogrel therapy may be longer than 1 year.
Balancing the Risks and Benefits of Antithrombotic Therapy
Bleeding and transfusion risk is high with current antithrombotic treatments, noted Frans Van de Werf, MD, University Hospital Gasthuisberg, Leuven, Belgium. Prof. Van de Werf suggested strategies for balancing the benefits and risks of long-term antithrombotic therapy for patients with NSTEMI or STEMI.
Approximately 15% of patients with NSTEMI require transfusions due to excess bleeding during their hospitalization [Yang J et al. JACC 2005]. Transfusions are associated with an increased risk in 30-day mortality in patients with NSTEMI (OR 3.94, 3.26–4.75) and in those with STEMI (OR 3.7; p<0.0001) [Rao SV et al. JAMA 2004; The APEX-AMI Investigators. JAMA 2007], although a causal relationship is difficult to establish.
Prof. Van De Werf offered several recommendations for balancing benefit and risk in this patient population. For example, he recommended performing invasive procedures only when indicated, and suggested considering radial artery access in patients at high risk for bleeding. Coronary artery bypass grafting should be performed after stopping clopidogrel for at least 5 days.
Prof. Van De Werf also suggested using fondaparinux or bivalirudin in patients at high risk for bleeding. Finally, limiting the use of upfront glycoprotein IIb/IIIa inhibitors to only high-risk NSTEMI patients may also reduce bleeding, although studies are conflicting regarding the potential loss in efficacy, and additional studies are ongoing [EARLY ACS – Giugliano. AHJ 2005;149:994–1002]. Antithrombotic agents should be dosed carefully, especially in elderly, female, or low-weight patients, and in those with renal failure to avoid overdosing these patients who are at increased risk of bleeding. [Alexander. JAMA 2005;294:3108–16]. Lastly, Prof. Van De Werf reminded the audience that use of a proton pump inhibitor in patients with a history of gastrointestinal bleeding is now recommended by the updated nSTE-ACS guidelines [Anderson et al. JACC 2007].
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.