

Summary
Women experience coronary artery disease (CAD) approximately 10 years later than men, but the gender advantage ends there. By a number of parameters, women tend to have poorer outcomes. Women with stable coronary disease have better survival than men. In contrast, outcomes after an acute myocardial infarction (MI) are worse in women, with higher mortality rates during hospitalization at 30 days and at 1 year and more non-fatal complications including recurrent MIs.
- coronary artery disease
- prevention & screening
- menopause
Women experience coronary artery disease (CAD) approximately 10 years later than men, but the gender advantage ends there. By a number of parameters, women tend to have poorer outcomes, speakers said at several sessions devoted to women and CAD.
Women with stable coronary disease have better survival than men. In contrast, outcomes after an acute myocardial infarction (MI) are worse in women, with higher mortality rates during hospitalization at 30 days and at 1 year and more nonfatal complications including recurrent MIs, said Leslee Shaw, MD, Emory University, Atlanta, GA.
Poorer outcomes in acute coronary syndromes (ACS) may be the result of differences in characteristics at presentation, underlying biology, and treatment bias. On average, women tend to be older at the onset of ACS; have more diabetes and hypertension; present with more atypical symptoms, thus delaying therapeutic interventions; and are more likely to have nonspecific or nontraditional biomarker patterns (more frequent T wave inversions and normal troponin levels, but higher levels of brain natriuretic peptide and C-reactive protein). On angiography, women typically have more nonobstructive CAD and less severe and less extensive obstructive disease. They also tend to have smaller and less severe infarcts, and preserved systolic function, yet more heart failure, Dr. Shaw said.
Carl Pepine, MD, University of Florida, Gainesville, FL, described how traditional risk factors and also conditions unique to women may contribute to their risks (Table 1).
Preclinical Conditions Leading to More Severe or Different Forms of Vascular Disease.
Dr. Pepine maintained that vascular biology of atherosclerosis may be affected by gender-related (eg, hormone-mediated) issues, leading to differences in clinical presentation and outcomes (Table 2). “A host of features support a hypercoagulable and prothrombotic state in women,” he said.
Coronary Vascular Conditions Leading to More Severe or Different Forms of Vascular Disease.
The tendency for women to have normal or nonobstructive coronary disease in ACS contributes to the lack of perception of risk after the acute event. In an analysis of patients with nonobstructive CAD in three major trials (Bugiardini R et al. Arch Int Med 2006;166:1391–1395), patients with non-ST-segment elevation ACS had a 12% risk for a cardiac event through 1 year. Patients with mild disease versus those with normal angiographic findings had worse outcomes. The combined endpoint of death, MI, revascularization, or unstable angina was reached by 15.1% in the mild disease group versus 9.4% in patients with normal coronaries (p=0.05), she noted.
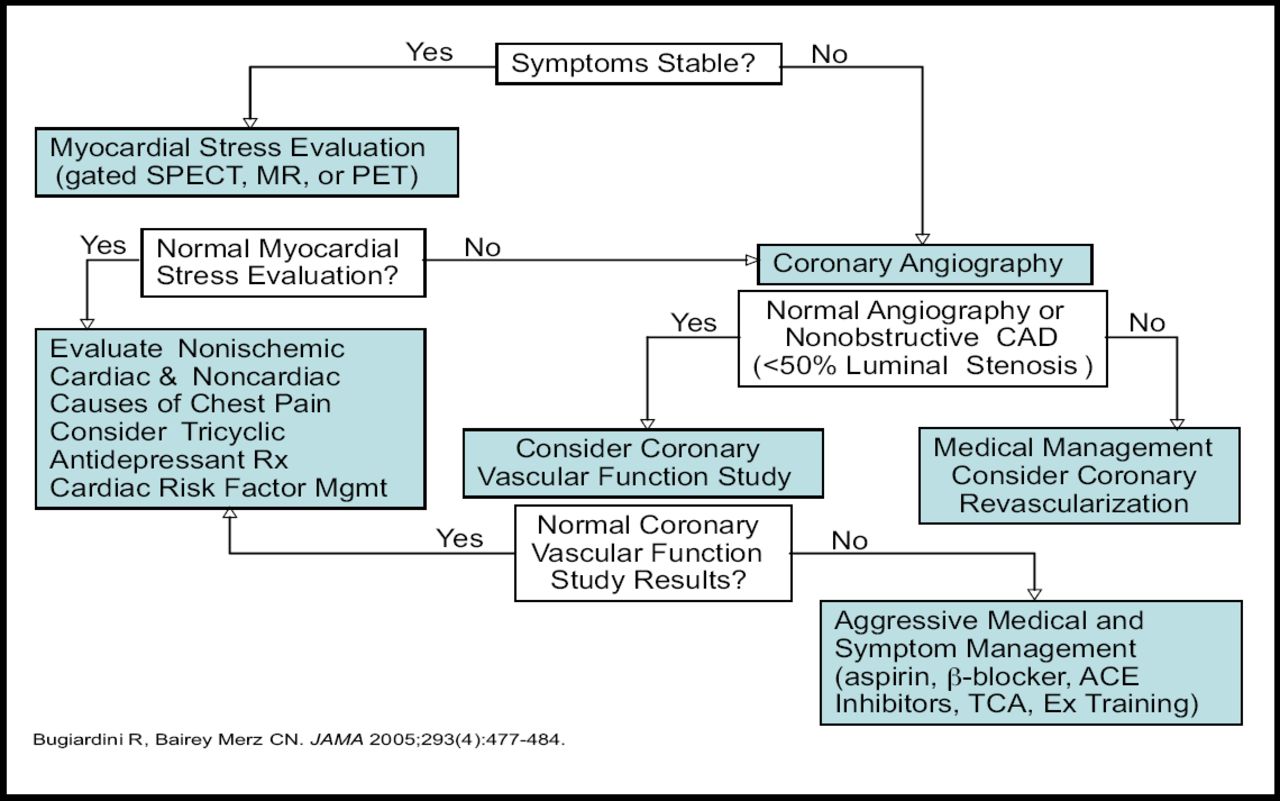
Women with nonobstructive disease, therefore, should be carefully assessed for the extent of atherosclerosis and coronary vascular function so that their true cardiovascular risk can be defined and the disease intensively managed, Dr. Shaw said (Figure 1).
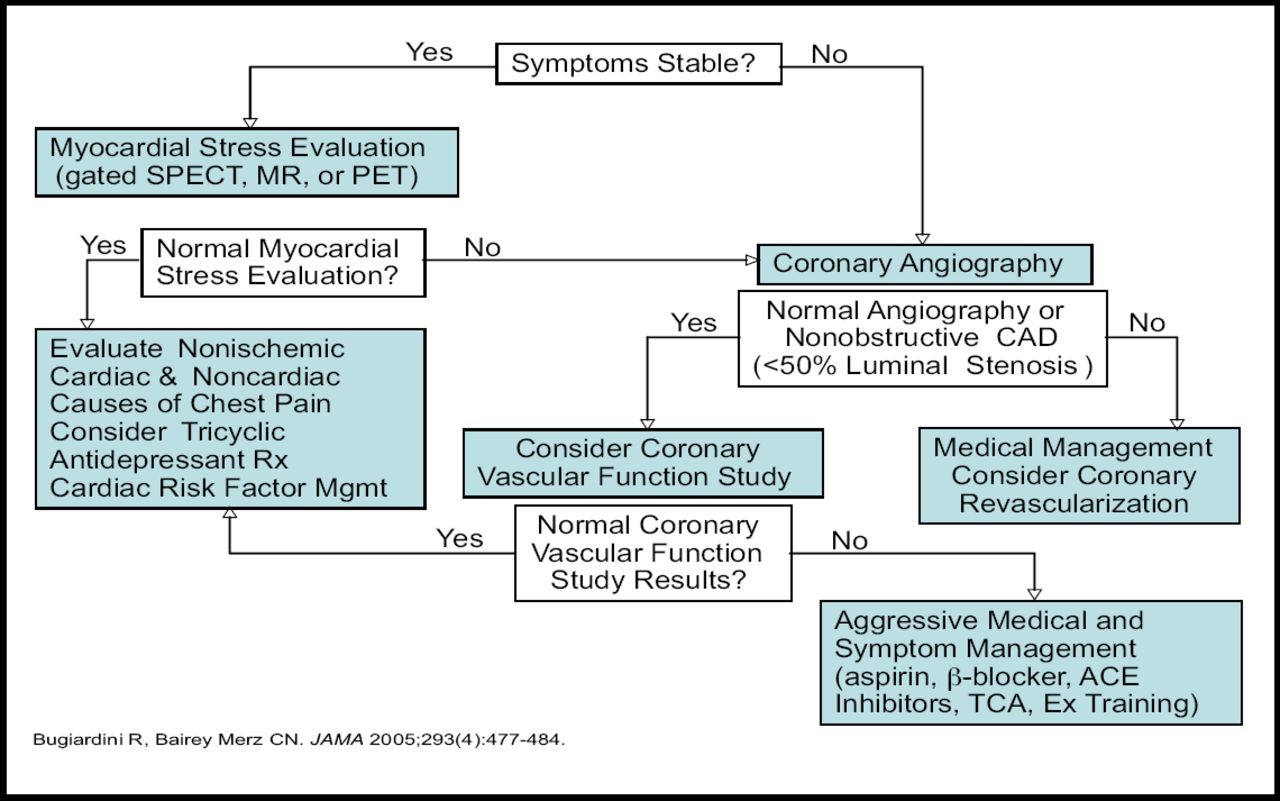
Management of Patients with Nonobstructive CAD.
Viola Vaccarino, MD, PhD, Emory University, Atlanta, GA, reiterated that because risk is perceived to be lower in women, a “higher risk burden” is required for diagnosis and therapy. “This leads to referral bias; to patients being sicker when diagnosed, hospitalized, and treated; and to less preventive treatment,” she said.
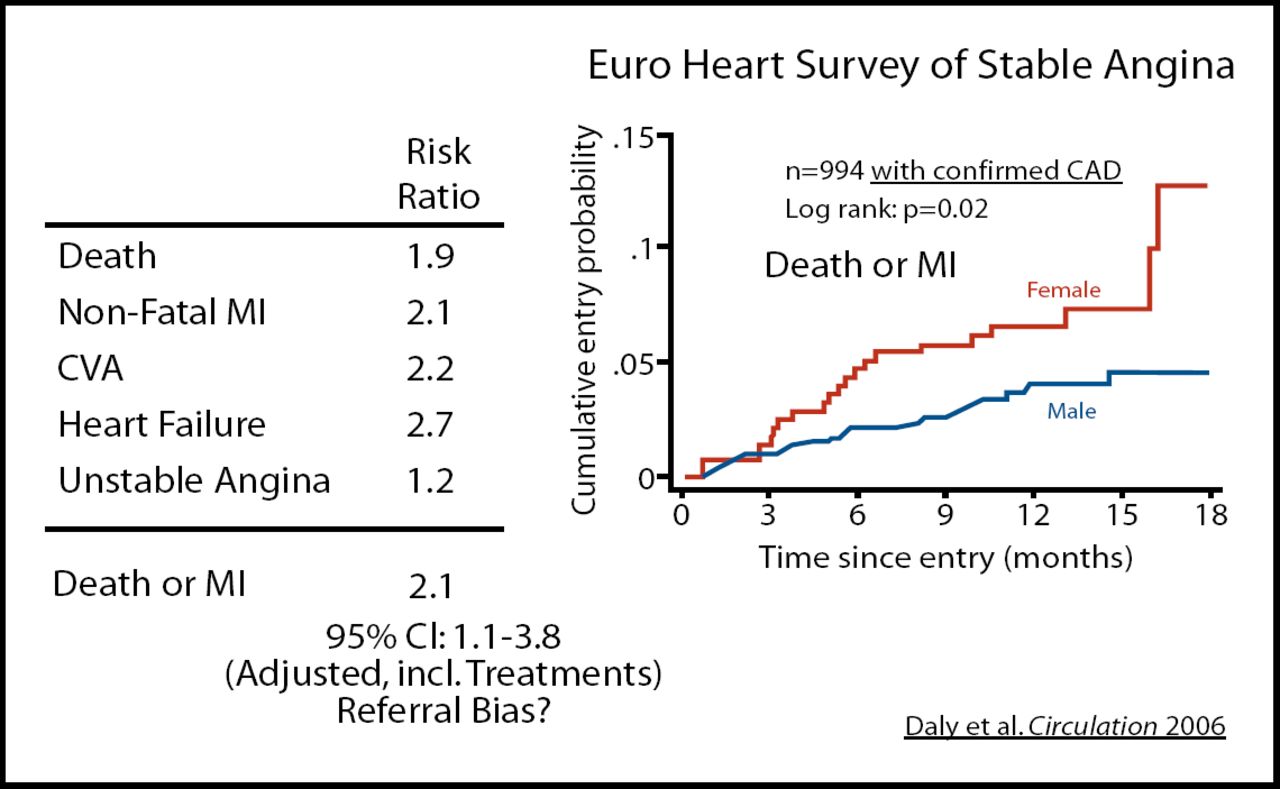
While MI is the most common initial manifestation of CAD in men, for women it is uncomplicated angina. Lower utilization of noninvasive diagnostic tests for angina in women can translate to delayed or absent treatment, disease progression, and worse outcomes. In the European Heart Survey of Stable Angina (Daly C et al. Circulation 2006;113:490–98), women were 14% less likely to be referred for angiography, 30% less likely to undergo revascularization, and significantly less likely to be put on antiplatelet therapy, statins, and beta blockers (p<0.001). This less aggressive therapy resulted in poorer outcomes and an increased risk of death or MI (p=0.02; Figure 2).
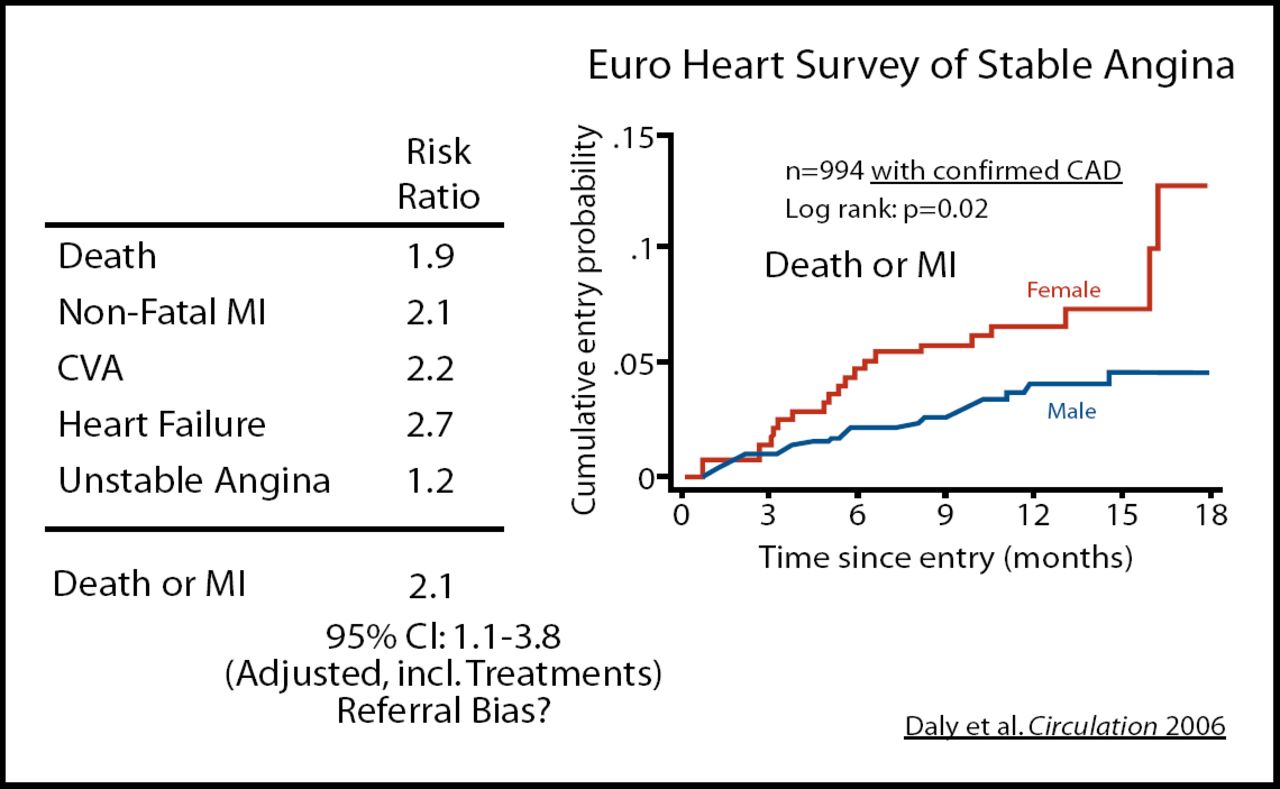
Clinical Course of Angina with Confirmed CAD, Women vs Men.
Effect of Estrogen
Estrogen is thought to be cardioprotective, based largely on the fact that women develop ischemic heart disease predominantly after menopause, but there are several biological reasons as well, according to Dr. Pepine. Estrogen interacts at the endothelial cell level to reduce reactive oxygen species, increase nitric oxide, relax vascular smooth muscle, suppress inflammation, and inhibit vascular smooth muscle cell proliferation.
The cardioprotective benefits of estrogen replacement therapy, however, have been difficult to prove. Jacques E. Rossouw, MD, National Heart, Lung, and Blood Institute (NHLBI), Bethesda, MD, reviewed current concepts about hormone therapy (HT) and CAD, concluding that “the most realistic way to view HT is that it has a narrow therapeutic range compared to other prevention strategies.” Maximum benefit (and least harm) is likely to occur with short-term use of HT for vasomotor symptoms immediately following menopause, with the long-term focus being on proven methods for CAD prevention, he said.
The randomized Women's Health Initiative (WHI) study (Writing Group for the WHI Investigators. JAMA 2002;288:321–333) concluded that estrogen plus progestin increased coronary heart disease in the first few years of use, and also increased stroke, blood clots, breast cancer, and dementia. Estrogen alone increased stroke, blood clots, and dementia but had no effect on heart disease or cancer. WHI investigators combined the randomized trial and observational datasets of the WHI and found less risk when HT was initiated within 10 years of menopause, versus more distantly (Table 3; Rossouw JE et al. JAMA 2007;297:1465–1477).
Risk of CHD with Hormone Therapy Stratified by Timing of Initiation of Treatment.
The lack of cardioprotection seen in the WHI study was in conflict with protective effects found in the observational Nurses Health Study (NHS), in which women may have initiated HT earlier (at menopause), before CAD develops. “Estrogen does not reduce existing atherosclerosis. In fact, it may destabilize vulnerable plaques and precipitate thrombosis,” he suggested. In the NHS, when time of onset of HT was considered, protection from HT was diminished in patients treated later after menopause.
Similar results emerged from the Women's Ischemia Syndrome Evaluation (WISE) study, reported at the AHA by George Sopko, MD, of the NHLBI. Among 654 postmenopausal women, the incidence of angiographically proven CAD was approximately 10% among women who started HT before age 45, compared with 25% of those starting HT after age 45 and over 40% for those never taking hormones.
Atherosclerotic Risk with Oral Contraceptives
Oral contraceptives, which contain more estrogen than HT, have been less studied. Investigators from Belgium reported that oral contraceptives may raise the risk for atherosclerosis 3,040% for every decade of use. In a study of 1,301 women, 81% of whom used oral contraceptives for an average of 13 years, the prevalence of carotid as well as femoral artery plaque (observed on ultrasonography) rose significantly for each decade of exposure, reported Ernst Rietzschel, MD, Ghent University, Ghent, Belgium.
“In the light of widespread and usually prolonged oral contraceptive use, oral contraceptives could be an important factor in the global atherosclerotic burden,” Dr. Rietzschel said, suggesting that clinicians closely monitor and control the classic risk factors.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.