

Summary
This article discusses the use of beta-blockers in the treatment of hypertension. Also discussed are the LIFE, ASCOT-LLA, ASCOT-BPLA, and ASCOT-CAFE trials, as well as European Society of Hypertension/European Society of Cardiology hypertension guidelines.
- hypertensive disease
Beta-Blockers: No Longer Preferred Therapy in Hypertension
“Newer drugs, especially in combination, have advantages over beta-blockers,” said Adrian J.B. Brady, MD, Glasgow Royal Infirmary, Glasgow, Scotland.
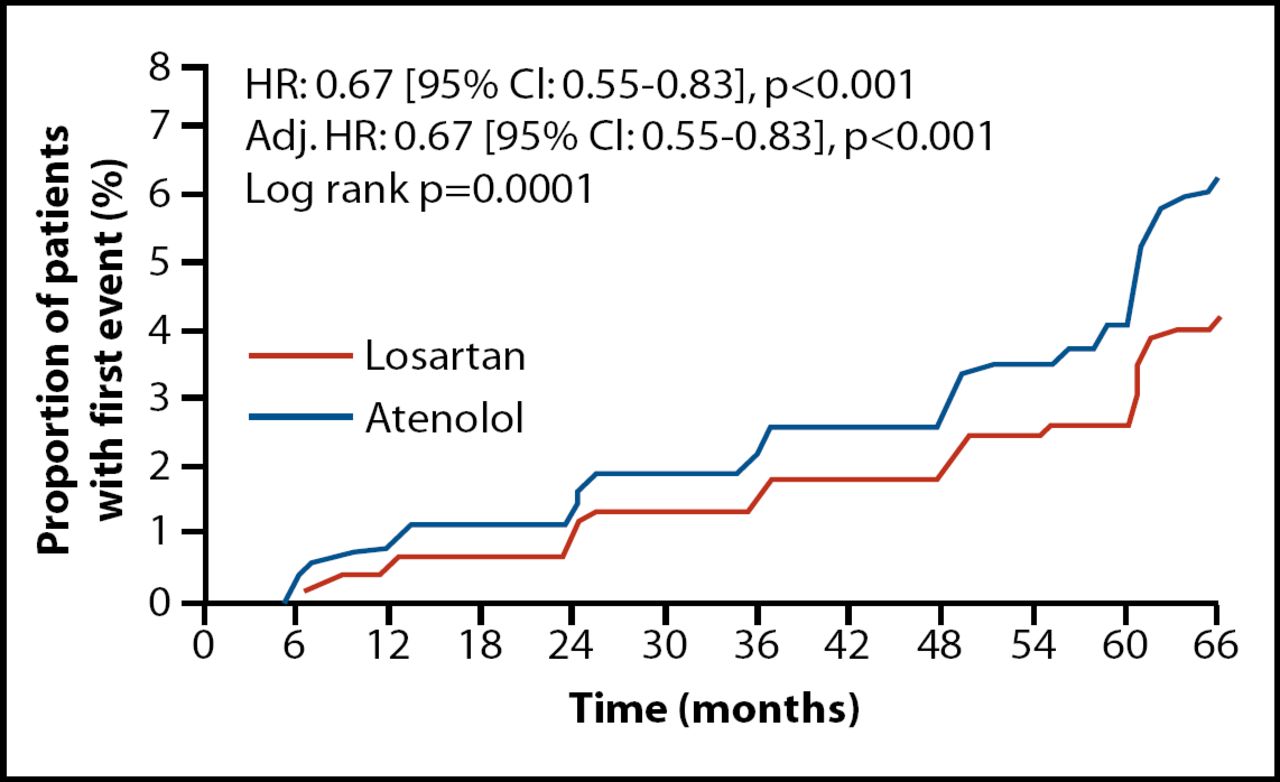
In several analyses of the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial, losartan-based therapy was better than atenolol-based therapy for a range of outcomes, including atrial fibrillation (AF) (Figure 1) [Wachtell K et al. JACC 2005]. The superiority of losartan over atenolol in AF was a surprising finding, given that beta-blockade has historically been recommended as first-line therapy to prevent AF and it is the preferred treatment for rate-control in established AF [Fuster V et al. JACC 2001].
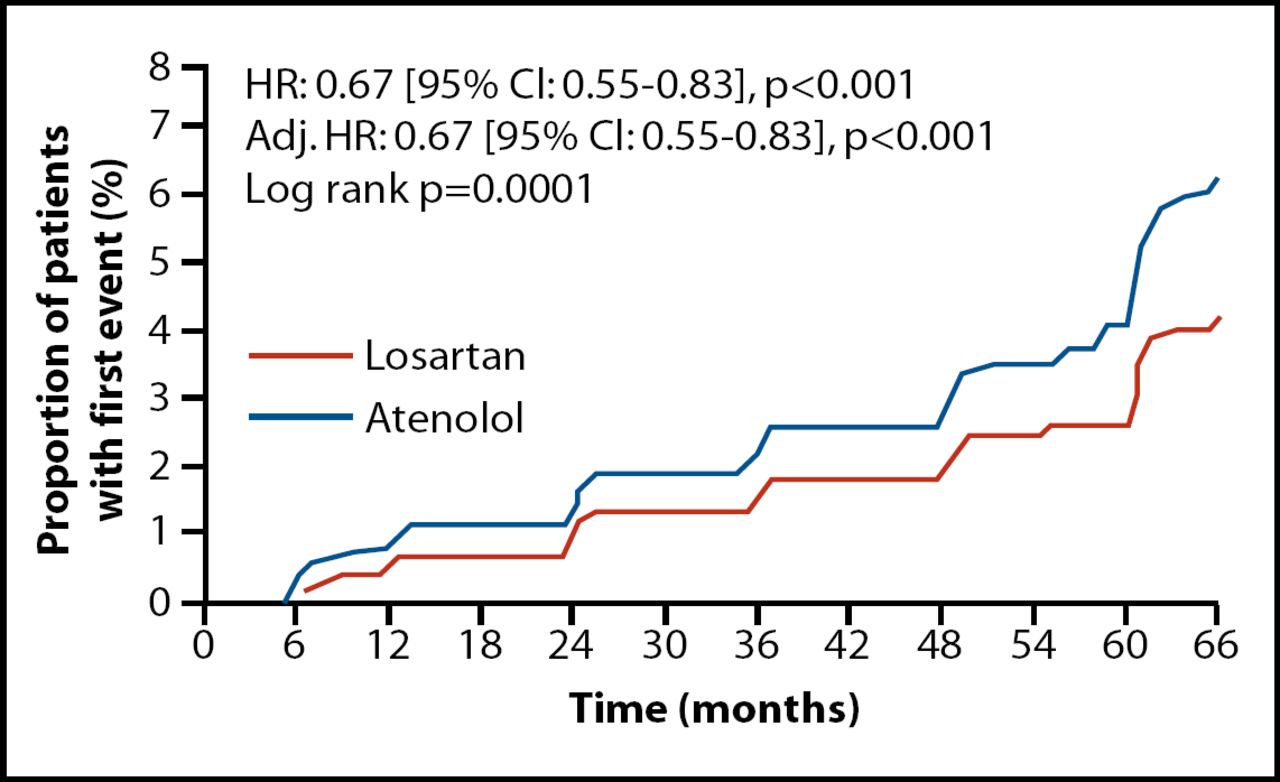
LIFE: New-Onset Atrial Fibrillation.
Reprinted from JACC, Wachtell K et al, copyright 2005, with permission from the American College of Cardiology.
In the Anglo-Scandinavian Cardiac Outcomes Trial - Lipid Lowering Arm (ASCOT-LLA), benefits associated with atorvastatin therapy in the amlodipine group were not observed in the atenolol group. In ASCOT-LLA, patients randomized to amlodipine or atenolol in the main ASCOT trial were further randomized to atorvastatin (n=5,168) or placebo (n=5,137). Among patients in the amlodipine group, atorvastatin reduced coronary heart disease (CHD) events by 53% (p<0.0001). In contrast, atorvastatin did not provide significant protection against CHD events in the atenolol group. Differences in blood pressure and lipid parameters between the amlodipine and atenolol treatment arms could not account for the differences in CHD outcome [Sever PS et al. Eur Heart J 2006].
“When we are treating multiple risk factors, such as hypertension and hyperlipidemia, beta-blockers may not be the preferred therapy for these individuals,” Prof. Brady said.
Beyond blood pressure-lowering, Prof. Brady emphasized the importance of other physiological effects when considering the benefits of different antihypertensive agents. Implications of these other physiological effects were illustrated when patients in the ASCOT-Blood Pressure Lowering (ASCOT-BPLA) arm were matched for blood pressure at several time points across the study. Creating a large cohort of patients with the same blood pressure allowed researchers to identify whether different agents produced different clinical outcomes beyond blood pressure-lowering. Compared with those in the atenolol group, patients in the amlodipine group had a 13% lower risk of all-cause mortality and coronary revascularization (HR 0.87; p=0.0177) and a 17% lower risk for fatal and nonfatal stroke (HR 0.83; p=0.0147) that was unaccounted for by improvements in blood pressure alone [Poulter NR et al. Lancet 2005].
Prof. Brady noted that different antihypertensive agents have different effects on central blood pressure. Indeed, another subanalysis of ASCOT, the Conduit Artery Function Evaluation (ASCOT-CAFE) trial, demonstrated that different antihypertensive agents can have substantially different effects on central aortic pressures and hemodynamics despite similar impacts on brachial blood pressure. In ASCOT-CAFE, patients in the amlodipine and atenolol treatment arms had similar brachial systolic blood pressures, with an average difference of 0.7 mm Hg between groups (p=0.2). Despite this similarity, patients in the amlodipine group had significantly greater reductions in central aortic pressures, including central aortic systolic blood pressure (4.3 mm Hg; p<0.001) and central aortic pulse pressure (3.0 mm Hg; p<0.0001), compared with the atenolol group.
Differences in central pressure have major clinical implications. In ASCOT-CAFE, central pulse pressure was significantly associated with the composite endpoint of total cardiovascular events and procedures and development of renal impairment (p<0.05, adjusted for baseline variables) [Williams B et al. Circulation 2006]. This finding provides further support for the idea that beta-blockers lack important cardioprotective features present in other antihypertensive agents, Prof. Brady said.
The movement away from beta-blockers as preferred blood pressure agents is reflected in the updated hypertension guidelines published by the National Institute for Health and Clinical Excellence (NICE) and the British Health Service. Based on recent data favoring other antihypertensive agents, beta-blockers are no longer preferred as a routine first-line therapy for hypertension. Instead, beta-blockers are recommended as a fourth option behind ACE inhibitors, calcium channel blockers, and thiazide-type diuretics.
Beta-Blockers: Still Valuable Therapy in Hypertension
Taking the opposing view, Björn Dahlöf, MD, PhD, University of Göteborg, Sweden, argued in his presentation that beta-blockers still play an important role in the treatment of hypertension.
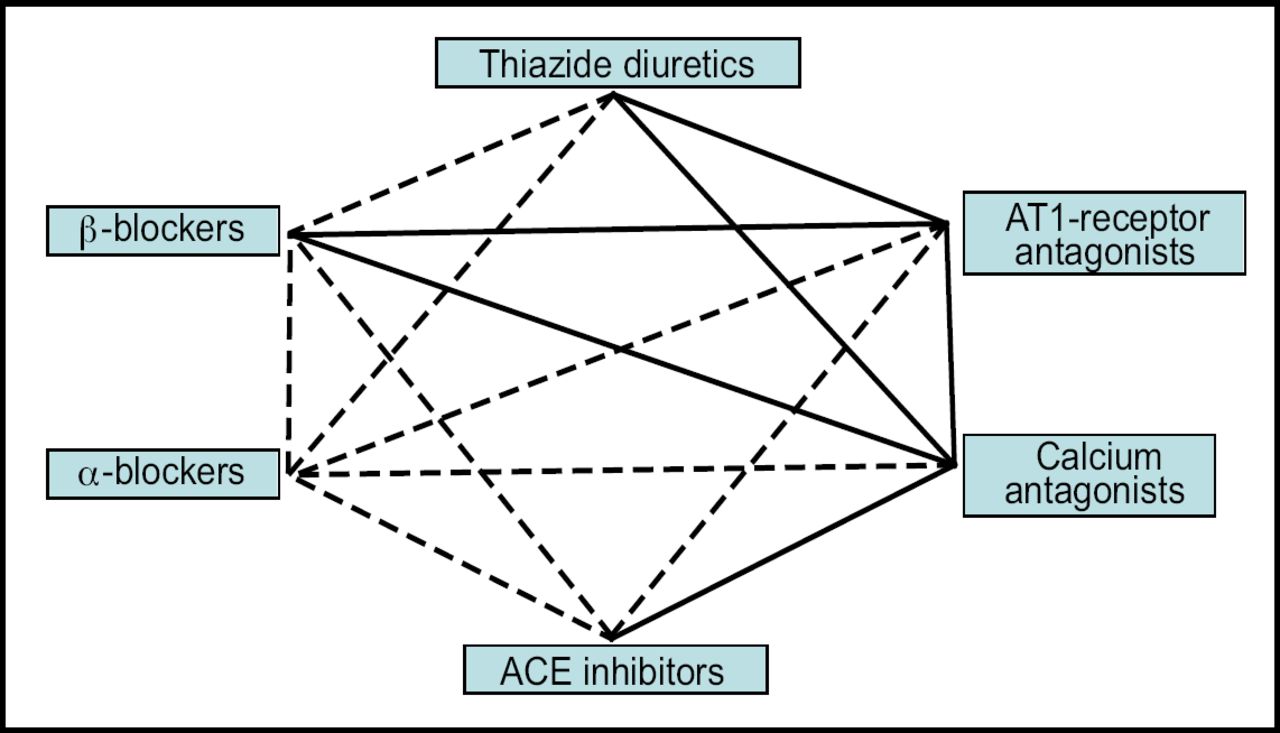
“One of the reasons we have been unsuccessful in treating hypertension is that we have not agreed on first-line therapy in the guidelines,” Prof. Dahlöf said. As examples, he pointed to the 2006 NICE guidelines and the 2007 European Society of Hypertension (ESH)/European Society of Cardiology (ESC) hypertension guidelines (Figure 2).
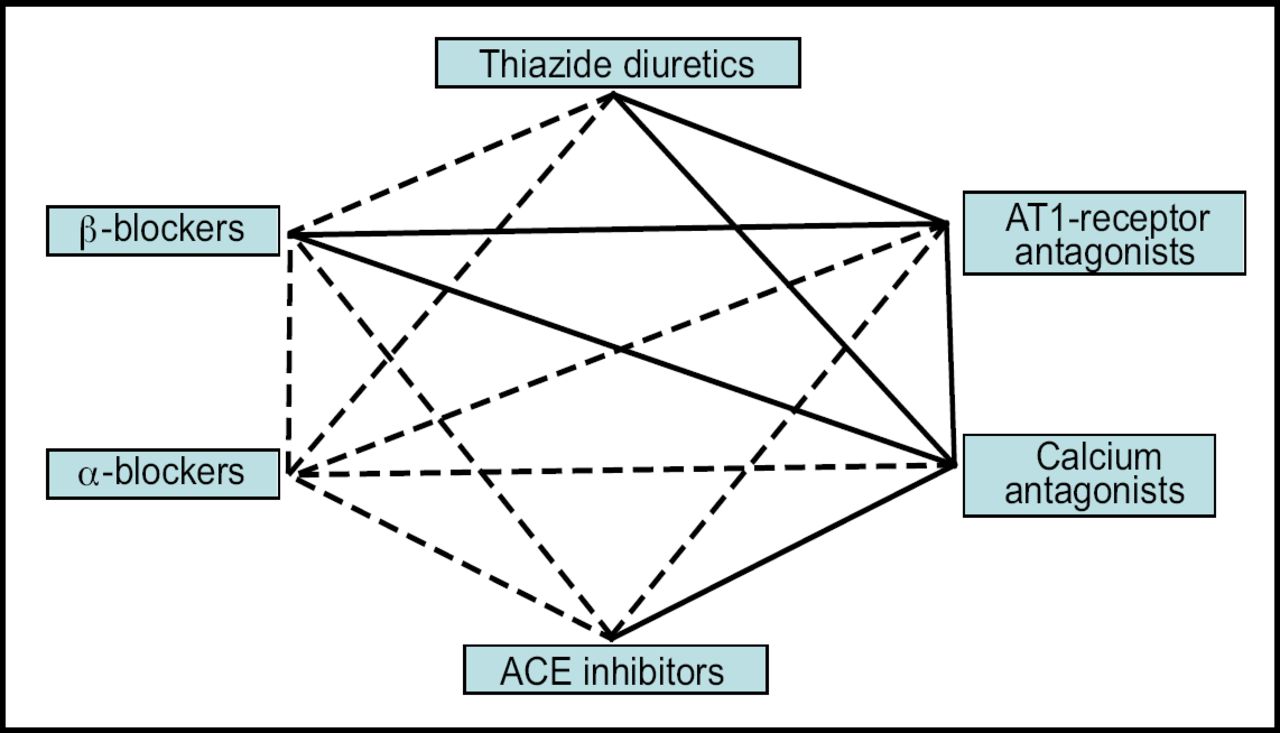
2007 ESH/ESC Guidelines: Antihypertensive drug combinations.
ESH=European Society of Hypertension
ESC=European Society of Cardiology
Reprinted with permission from Eur Heart J, Mancia G et al, copyright 2007.
Preferred combinations for the general hypertensive population are represented as thick lines.
Frames indicate classes of agents with proven benefits in controlled intervention trials. Whereas the 2006 NICE guidelines list beta-blockers as fourth-line agents, the 2007 ESH/ESC hypertension guidelines position beta-blockers much more prominently [Mancia G et al. Eur Heart J 2007]. Specifically, the 2007 ESH/ESC hypertension guidelines note:
-
The main benefits of antihypertensive treatment are due to lowering of blood pressure per se, and are largely independent of drugs employed
-
Thiazide diuretics, beta-blockers, calcium antagonists, ACE inhibitors, and angiotensin receptor antagonists can adequately lower blood pressure and significantly and importantly reduce cardiovascular outcomes
-
These drugs are thus all suitable for initiation and maintenance of antihypertensive treatment as monotherapy or in combination with each other
-
Beta-blockers are listed as favored agents in patients with previous MI, angina, permanent AF, tachyarrhythmia, and glaucoma
In addition to their blood-pressure-lowering effects, beta blockers provide other cardioprotective benefits in select patient subgroups. For example, a meta-analysis of four intravascular ultrasonography trials showed that beta-blockers slow the progression of coronary atherosclerosis in patients with known coronary artery disease (n=1,515) [Sipahi I et al. Ann Intern Med 2007]. Therefore, beta-blockers may play an important role in overall cardiovascular risk reduction.
Antihypertensive research is rapidly evolving, and Prof. Dahlöf acknowledged that the focus of research in blood pressure control is moving beyond traditional agents. Given the results of LIFE and other recent trials that have demonstrated the superiority of newer agents over atenolol, atenolol is no longer an appropriate reference drug for future trials of cardiovascular risk in hypertension, he said. However, he argued that beta-blockers should be judged on an individual molecular basis, adding that newer beta-blockers still have a role in hypertension research.
“Although beta-blockers are no longer the preferred first-line agents in the treatment of uncomplicated hypertension, these agents still have a place in the therapeutic armamentarium,” Prof. Dahlöf concluded. “Beta-blockers are needed in patients with special conditions and indications.”
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.