

Summary
Diagnostic imaging utilization continues to grow in the United States. In one report, the number of inpatients getting magnetic resonance imaging or computed tomography scans doubled from 1996 to 2002 [Beinfield & Gazelle. Radiolog 2005]. As the use and associated health care costs of imaging diagnostics continues to rise, it is important that clinicians select the correct test for each patient. Several experts in the fields of cardiac imaging presented their insight into the advantages of different imaging modalities in various cardiac patient populations.
- cardiac imaging techniques
- imaging modalities
Diagnostic imaging utilization continues to grow in the United States. In one report, the number of inpatients getting magnetic resonance imaging (MRI) or computed tomography (CT) scans doubled from 1996 to 2002 (Beinfield & Gazelle. Radiology 2005). As the use and associated health care costs of imaging diagnostics continues to rise, it is important that clinicians select the correct test for each patient. Several experts in the fields of cardiac imaging presented their insight into the advantages of different imaging modalities in various cardiac patient populations.
Fundamentals of Delayed Gadolinium Enhancement in MI Visualization
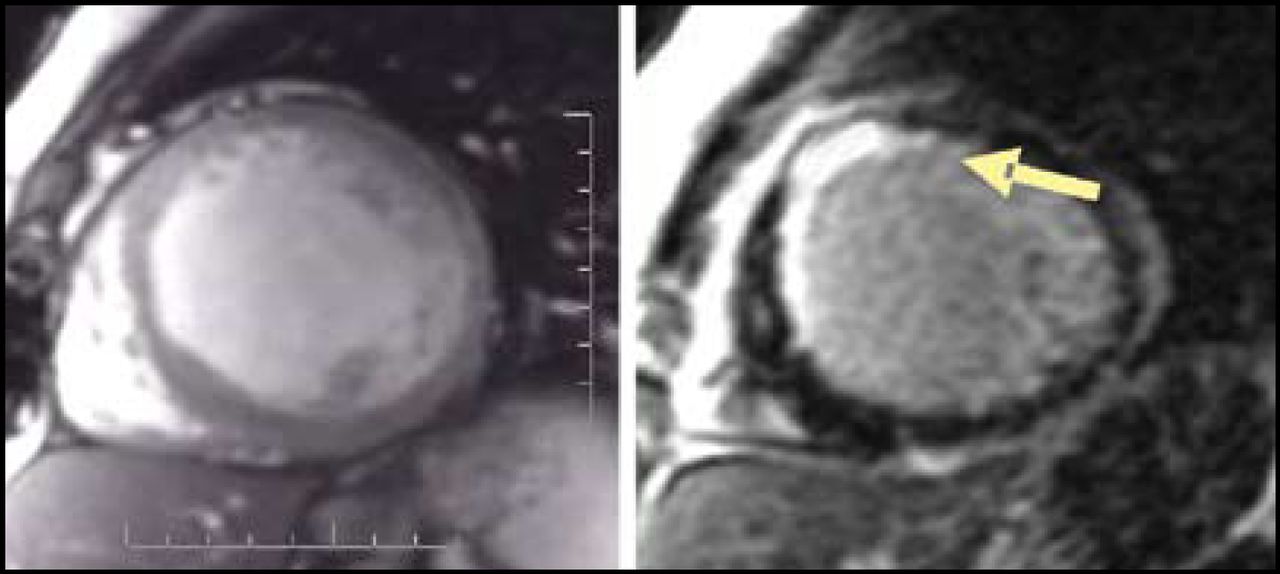
David Bluemke, MD, PhD, Johns Hopkins University, Baltimore, MD, presented a basic overview of late gadolinium enhancement (LGE) MRI in patients with myocardial infarction (MI). After gadolinium administration, there is an initial intense signal throughout the myocardium. In patients with normal kidney function, the contrast agent is cleared fairly rapidly from the heart tissue. When using this technique to visualize an MI, the initial images tend not to clearly depict the area of infarction. However, because scar tissue retains gadolinium for much longer than non-scarred tissue, images taken 10–20 minutes after injection show accumulation of gadolinium in the areas of necrosis, resulting in a contrast between scarred and non-scarred tissue (Figure 1). In addition to its high correlation with pathologic parameters, MRI with gadolinium offers a key advantage in that the difference in signal between diseased and normal tissue can be manipulated to produce a clearer image. “With CT, we don't have that ability to accentuate the contrast-to-noise ratio” said Dr. Bluemke.
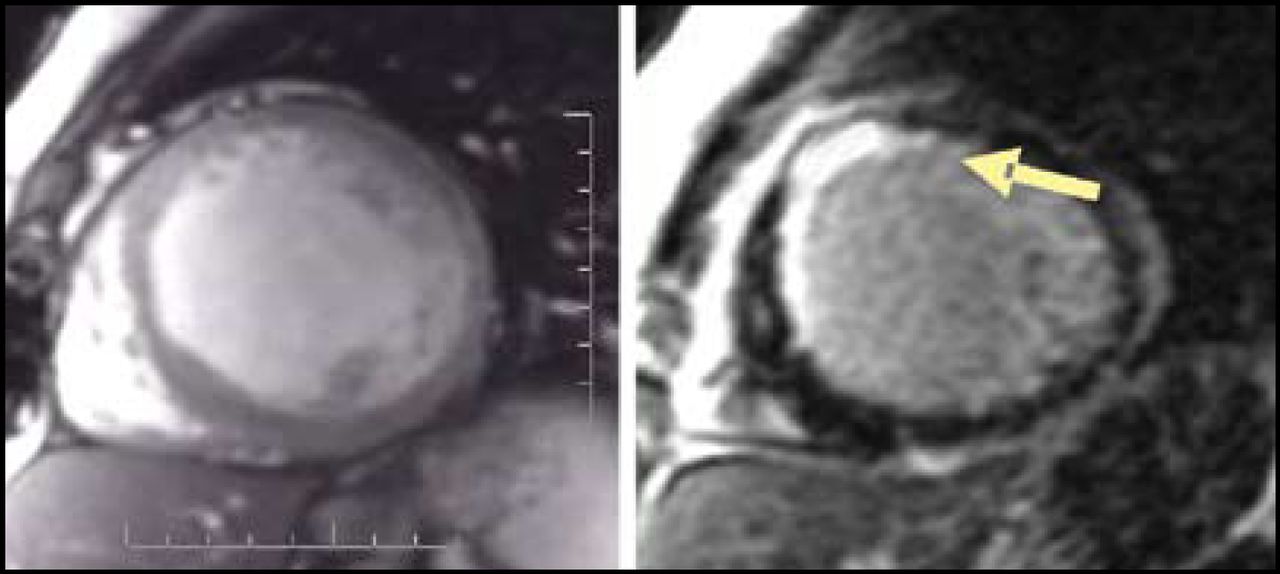
72-Year-Old Female with Congestive Heart Failure, Known Coronary Artery Disease: MRI Cine and Late Gadolinium Enhancement Images.
Another advantage of LGE MRI is the short duration of the procedure—while positron emission tomography takes approximately 4 hours to be completed, an MRI can be performed in 30 minutes. Dr. Bluemke reminded the audience that patients presenting with acute MI may not demonstrate scar enhancement initially. “There's actually a lot of variation depending on the status of the artery that's feeding that territory,” explained Dr. Bluemke, but gadolinium eventually diffuses into the scar. According to Dr. Bluemke, relating outcomes data to myocardial scars as well as the relationship between cell death and scar formation is an area of future research.
Appropriate Patient Selection in Cardiac MRI
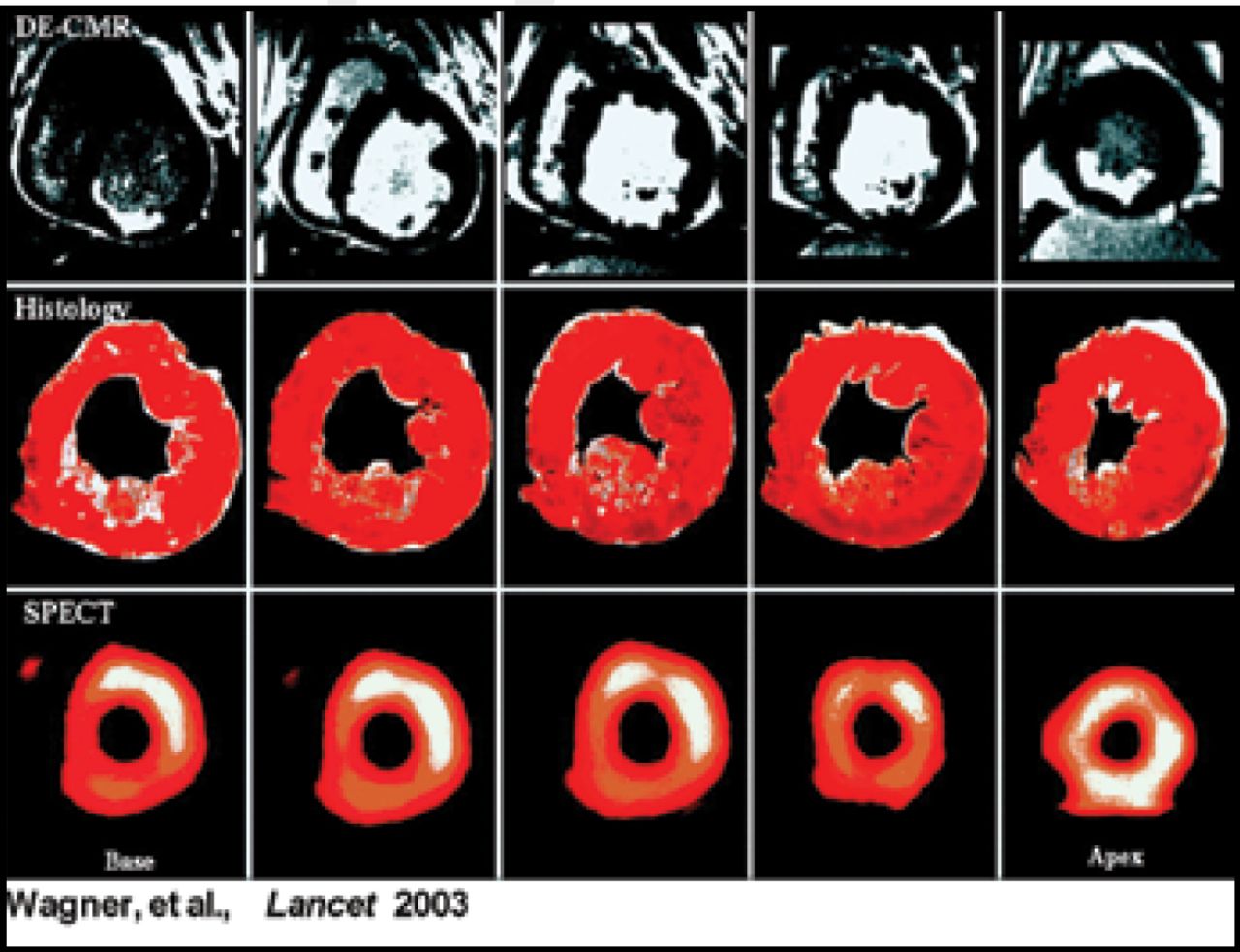
According to W. Gregory Hundley, MD, Wake Forest University School of Medicine, Winston-Salem, NC, stress cardiac MRI (CMR) has advantages over stress echocardiography. “At our institution, more than 3,000 patients per year were referred for stress echocardiography, but due to poor acoustic windows, 5–25% of them were not well-suited for the exam,” noted Dr. Hundley. This obviously led to treatment delays and in some cases longer hospital stays. Nagel et al published a study that demonstrated superior specificity, sensitivity, and positive and negative predictive values of CMR compared with stress echocardiography (all p<0.05; Circulation 1999). CMR offers a more detailed image of cardiac tissue since the spatial resolution of delayed enhancement CMR is much greater than that of single photon emission computed tomography (SPECT) (Figure 2). “This is a very powerful technique and is very robust. It correlates very nicely with infarcts in pathological specimens. In addition, it is much more accurate in identifying small subendocardial infarcts than radioisotope imaging,” commented Dr. Hundley.
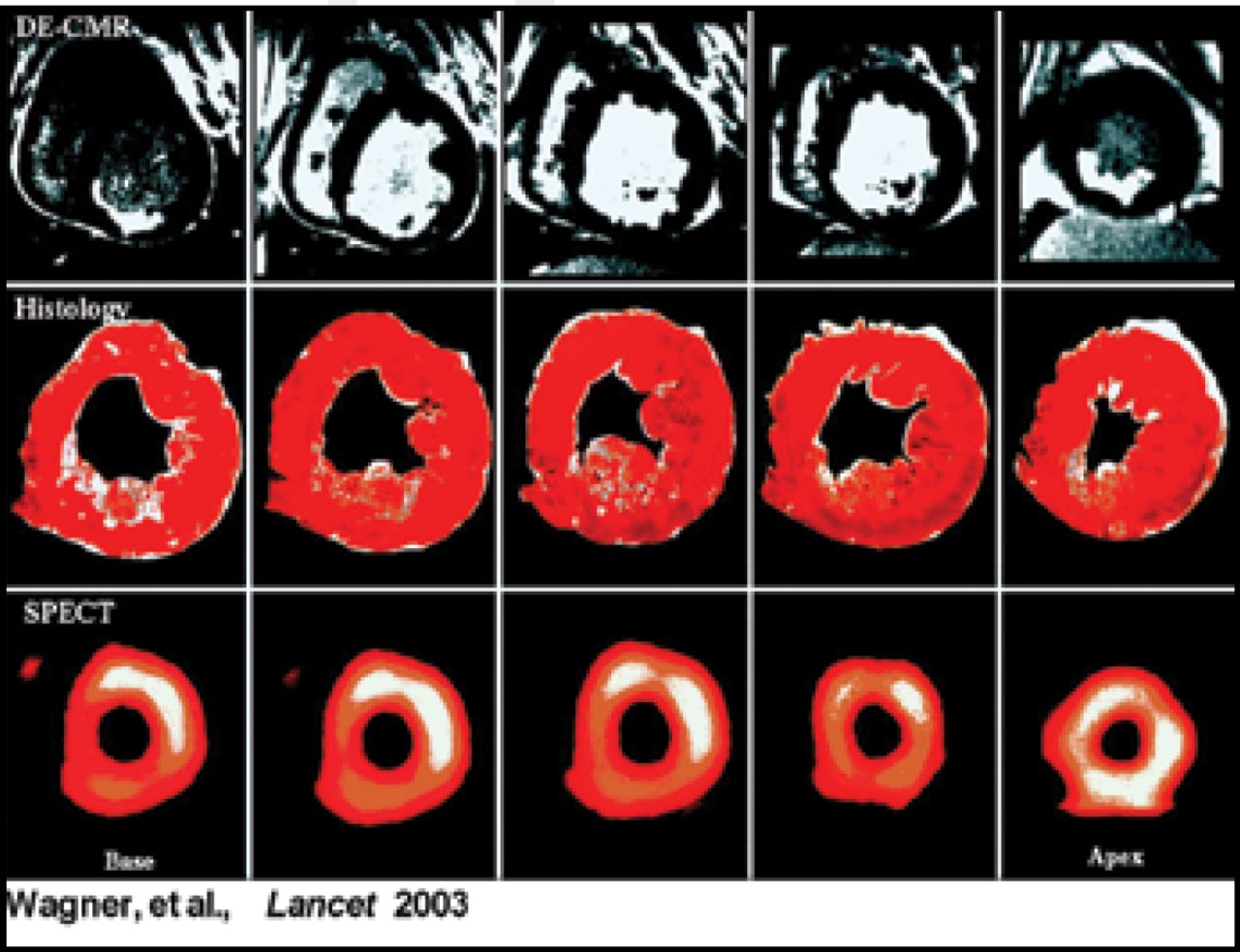
Heightened Accuracy Due to Enhanced Spatial Resolution.
A recent study by Kwong et al (Circulation 2006) demonstrated the prognostic value of delayed enhancement CMR. A total of 195 patients with no history of MI underwent CMR and LGE in order to assess left ventricular (LV) function and the presence of myocardial scarring. Patients were followed for 16 months, and 31 patients (18%) experienced major adverse cardiac events (MACE), including 17 deaths. The presence of LGE was strongly associated with increased risk of MACE (HR 8.29, 95% CI, 3.92–17.5) and cardiac mortality (HR 10.9, 95% CI, 3.75-=31.9).
The images generated by CMR are easily interpreted, which may lead to better education of patients regarding their condition. The best candidates for CMR include patients who cannot undergo invasive imaging modalities, require urgent chest pain evaluation, have LV hypertrophy, abnormal LV ejection fraction, or unexplained heart failure. “I believe that cardiac imaging specialists will move away over the next 10 years from being clinicans who are trained and isolated in MR, echo, or nuclear imaging and we will have an understanding of all the processes, the expertise, and the ability to read images from all three imaging modalities,” summarized Dr. Hundley.
Does Echocardiography still have a Role?
There is obviously a great deal of excitement regarding newer imaging modalities and contrast agents, but this does not mean that echocardiography no longer has a place in cardiac imaging. In use since the 1950s, echocardiography continues to be a mainstay of heart imaging. Margaret Redfield, MD, Mayo Clinic, Rochester, MN, reviewed the emerging contributions of echocardiography in the management of patients with advanced systolic heart failure. Patient selection is vital in the success of left ventricular assist device therapy (LVAD), and echocardiography is a useful tool in this selection process since it is widely available, portable, extremely safe, and can integrate structural and functional cardiac information. In Dr Redfield's opinion, clinicians managing patients with heart failure often rely too much on symptoms and risk scores, and they should supplement this information with the broad range of reliable data that can be obtained from modern echocardiographic techniques.
Despite the long track record of echocardiography, new applications for it, such as the determination of ventricular dyssynchrony, continue to be identified. In patients who undergo cardiac resynchronization therapy (CRT), approximately 70% will experience a decrease in symptoms, and 55% of that group will demonstrate reverse remodeling. “It's been hypothesized that the main reason patients don't respond to CRT and don't experience reverse remodeling is that some patients, despite having a wide QRS on their ECG, may not have electromechanical dyssynchrony,” said Dr. Redfield. This led to the question of what would happen if CRT was limited to patients with evidence of dyssynchrony. In a recently published study, echocardiography was used to successfully predict reverse remodeling. Specifically, measures of tissue Doppler longitudinal velocity were predictive of reverse remodeling (Yu et al. Am J Cardiol 2007). In the large, multicenter Predictors of Response to CRT (PROSPECT) trial, however, standard echocardiography and tissue Doppler did not predict clinical response to CRT (Chung et al. European Society of Cardiology Annual Meeting 2007). “We need to understand more about the physiology associated with CRT so that we can target therapies for those patients most likely to benefit from them,” summarized Dr. Redfield.
Using Coronary Computed Tomography in the Emergency Room
Gilbert Raff, MD, William Beaumont Hospital, Royal Oaks, MI, believes that certain patients can benefit from the use of coronary computed tomography angiography (CTA) when presenting with acute chest pain. “It's important that we emphasize that patients with obvious ischemia or infarction by ECG or enzymes don't belong in the CTA lab,” warned Dr. Raff. Recent meta-analyses, however, have shown that CTA has a very high negative predictive value. “It is extremely reliable for the exclusion of disease, even mild or moderate disease that might escape evaluation by stress testing,” said Dr. Raff.
A randomized, controlled clinical trial of the use of multi-slice CT (MSCT) in the evaluation of acute chest pain was conducted by Dr. Raff and colleagues (Goldstein et al. JACC 2007). Low-risk patients presenting with chest pain were randomized to either an MSCT protocol or a standard of care (SOC) protocol. In the MSCT protocol, patients with normal results were sent home. Those with intermediate results underwent a nuclear stress study; if normal they were discharged, and if abnormal they were sent for coronary angiography. If the MSCT indicated a severe diagnosis, patients were sent for coronary angiography. In the SOC protocol, patients underwent a nuclear stress study. Those with normal results were discharged, and those with abnormal results underwent coronary angiography.
Ninety-nine patients were in the MSCT group, and 98 were randomized to the SOC arm. The investigators found that MSCT had conclusive results in 75% of the patients tested; the remaining 25% needed additional tests for a diagnosis to be made. The time to diagnosis was significantly lower in the MSCT group (3.4 hours vs 15.0 hours in the SOC group; p<0.001). The medical costs were also lower for the MSCT group ($1,586 vs $1,872; p<0.001), mostly driven by the reduction in length of stay. “Now we're into 2 years of follow-up and in the CT arm, none of the patients has had any evidence of coronary ischemia or cardiovascular events,” said Dr. Raff.
The most suitable patients for CTA are those with negative cardiac enzyme results, normal ECGs, and low-to-intermediate cardiovascular disease risk. Those with known coronary artery disease, ST changes, positive cardiac enzymes, or contrast allergies should not undergo CTA. “You need an experienced team and have to have coordination with the ER staff…the bottom line is that this does get your patients out of the ER quite quickly,” concluded Dr. Raff.
The array of imaging tools that cardiologists have at their disposal will no doubt continue to grow. Additional research will add to our understanding of the most accurate, safe, cost-effective, and efficient methods to gather information in specific patient populations.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.