

Summary
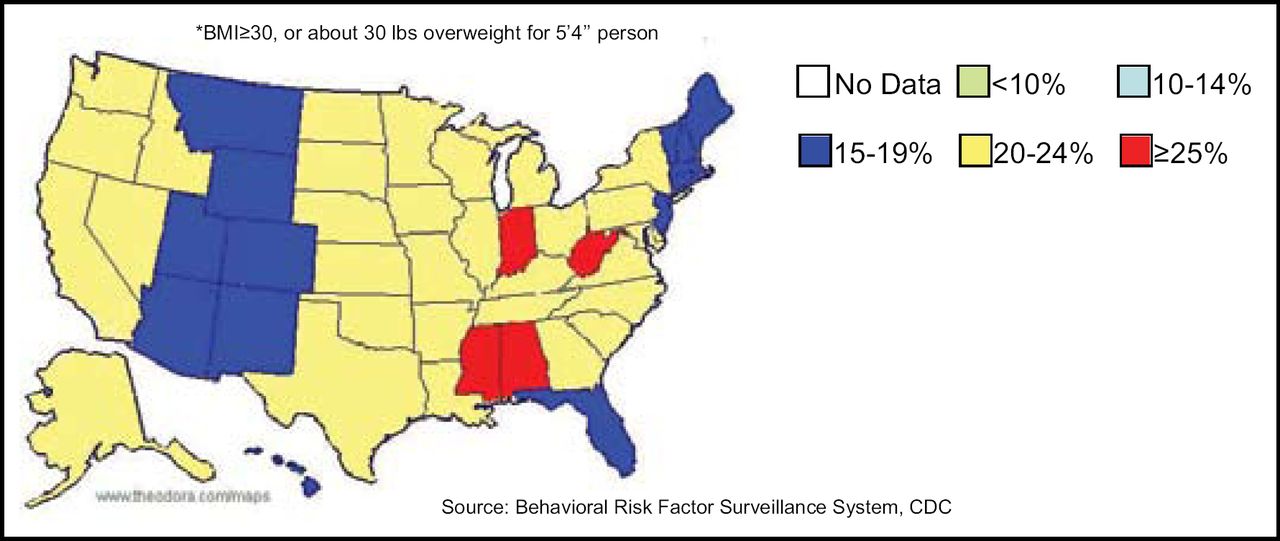
In a survey of the 50 US states in 1985, the highest rates of obesity reported were 10–14% per capita in 8 states. This number changed drastically in the last 30 years, with 4 of the 50 states reporting >25% obesity in 2003, and the vast majority of the remaining states reporting 20–24% obesity. This article gives an overview of obesity, its relationship to diabetes, and what this means to cardiologists.
- obesity
- diabetes mellitus
- lipid disorders
In a survey of the 50 US states in 1985, the highest rates of obesity reported were 10–14% per capita in 8 states. This number changed drastically in the last 30 years, with 4 of the 50 states reporting >25% obesity in 2003, and the vast majority of the remaining states reporting 20–24% obesity. Barbara V. Howard, PhD, Medstar Research Institute, Hyattsville, MD, gave an overview of obesity, its relationship to diabetes, and what this means to cardiologists. “This is an extraordinary change over a very short period of time,” said Dr. Howard. This problem is not isolated to the United States, as obesity rates are climbing worldwide. Why is this happening? Although a great deal of attention has been given to the Western diet, inactivity is also a huge culprit. Current lifestyles involve much less physical activity than in previous times.
It is critical that glucose levels in cardiac patients be managed appropriately. Data from the CARDINAL (Complement and ReDuction of INfarct size after Angioplasty or Lytics) highlights the importance of glucose levels in coronary disease. This study found that nondiabetic patients with acute myocardial infarction (MI) who had high glucose levels at baseline and whose levels remained elevated had higher mortality (Goyal et al. Eur Heart J 2006). Because of the escalation of diabetes prevalence, it is projected that contribution of diabetes to cardiovascular death will rise from 21% in 1999 to 29% in 2025 (Figure 1). “This is not just an epidemiologic problem, it's translated into the patients you're seeing,” noted Dr. Howard.
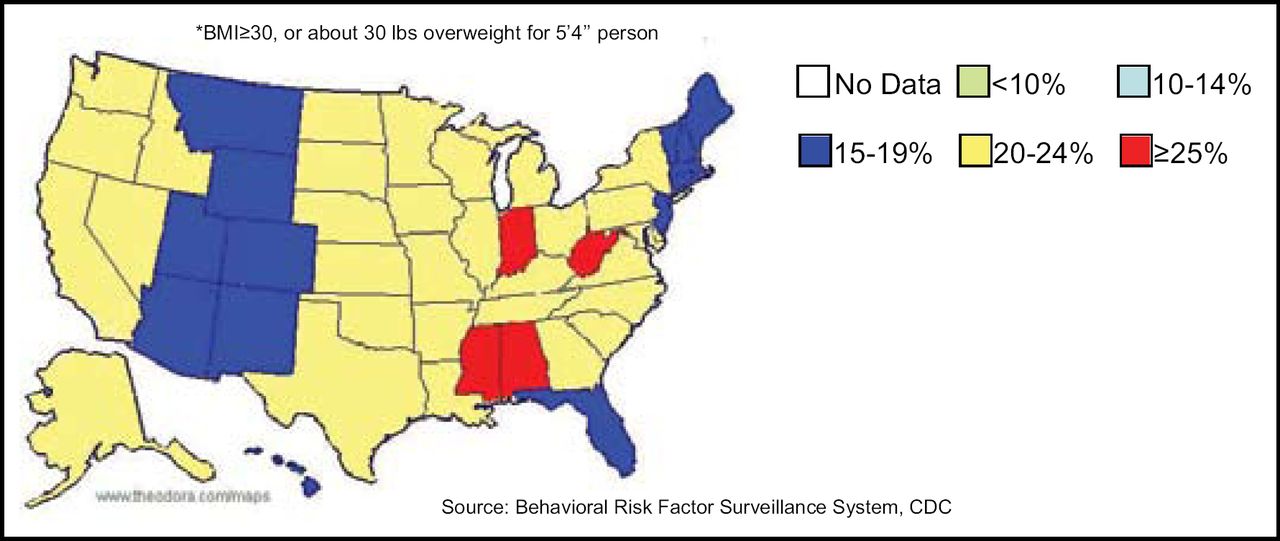
Obesity Trends Among US Adults.
Daniel Kelly, MD, Washington University, St. Louis, MO, presented the basic metabolic mechanisms of the diabetic heart. “Of the four major disease killers in the US today [heart disease, diabetes, cancer, stroke] diabetes is the only one that has increasing age-adjusted death rates” said Dr. Kelly in his introductory remarks. Indeed, cardiovascular disease (CVD) remains the leading cause of death in people with diabetes. In addition to atherosclerosis and hypertension that often accompany diabetes, there is myocardial disease as well. This is illustrated by the fact that diabetic patients have a much graver prognosis following an acute MI than nondiabetic patients. “Traditional secondary cardiac therapies we are giving patients following myocardial infarction are not as effective in the diabetic population,” said Dr. Kelly.
One thought is that the accumulation of fat in the heart affects CVD in diabetic patients. “This really is a problem of accounting, that there are more calories coming in than can be expended,” said Dr. Kelly. Once storage in the adipose tissue is exceeded, other organs (including the heart) begin storing fat. It is possible that this storage of fat in the heart muscle impacts the function of the heart in diabetic patients. The peroxisome proliferator activated receptor alpha (PPAR-α) promotes the transport and oxidation of fatty acids in the heart. This has led researchers to hypothesize that chronic activation of PPAR-α may be to blame in the problems of the diabetic heart. This idea has been explored using a transgenic mouse model (MHC PPAR-α), whereby the mice have chronic expression of PPAR-α. “Many of the signatures of the diabetic heart were recapitulated in this animal model…the hearts ran on fat,” said Dr. Kelly. When more fat was added to the mouse diet, additional cardiac dysfunction was observed (Finck et al. J Clin Invest 2002; Finck et al. Proc Natl Acad Sci USA 2003). These mice were subsequently bred with mice that had reduced cellular fat transport, the hypothesis being the inability to transport fat would “rescue” the heart from lipotoxicity. The results demonstrated that this was the case (Yang et al. Circ Res 2007). “These types of studies have demonstrated to us that 1) the importance chronically programming that is involved in metabolism of the diabetic heart, and 2) the increase of fatty acid delivery that occurs in the diabetic state. It raises the question of whether we should be thinking of modulating fatty acid and lipid delivery to the heart in the individual who has a combination of heart disease and diabetes,” summarized Dr. Kelly.
Darren McGuire, MD, University of Texas Southwestern Medical Center, Dallas, TX, discussed the treatment goals of diabetic patients in 2007. The rising increase in diabetes is a “dramatic public health catastrophe and we are at the forefront of that,” said Dr. McGuire. “We have completely engineered physical activity out of our daily lives,” he noted. One therefore has to make a conscious choice to take the stairs instead of the elevator, and walk more during the day. He suggested that attendees use the pedometers given to them at the meeting, and encourage their patients to do so as well.
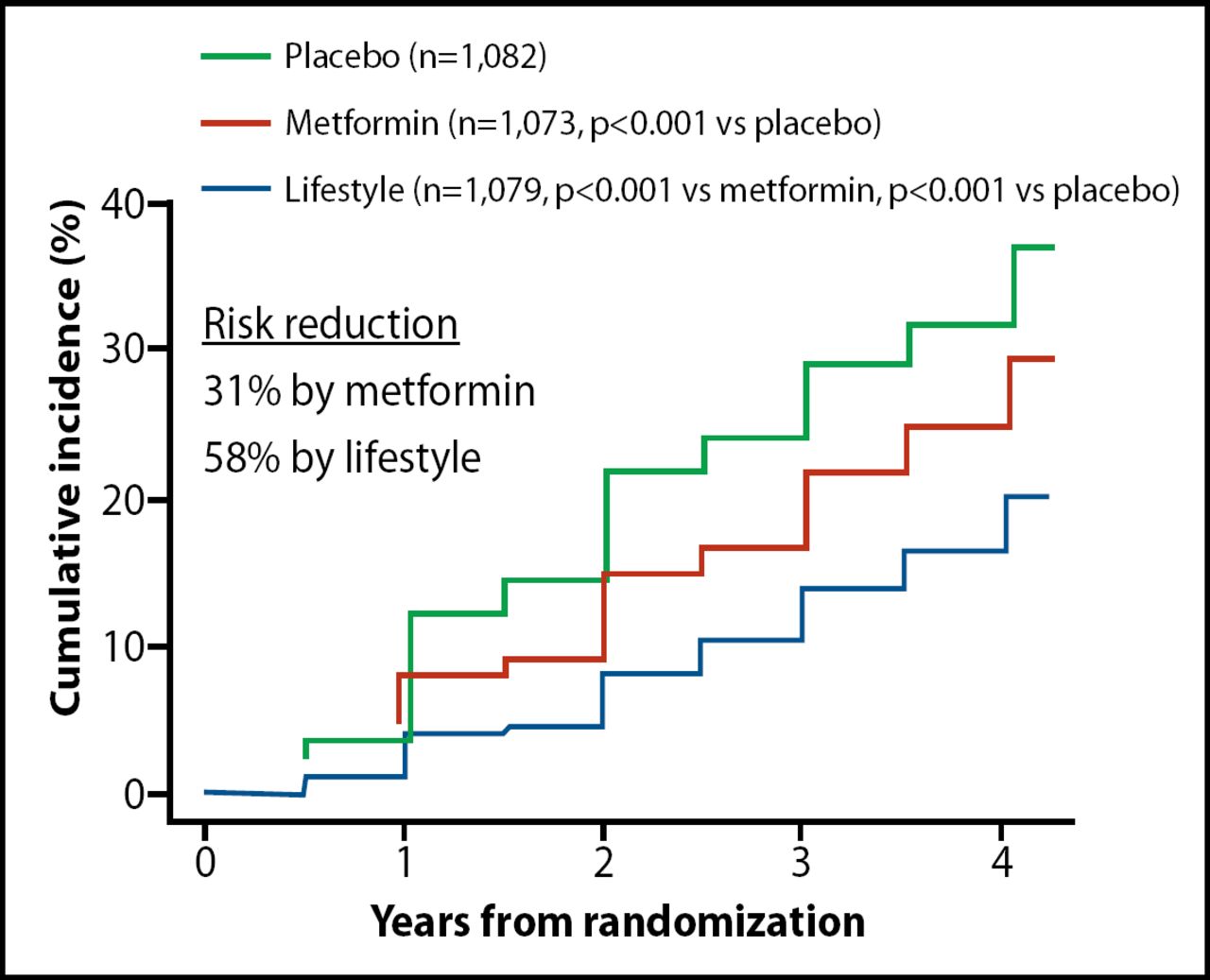
The number one treatment goal is diabetes prevention, and lifestyle interventions have demonstrated that they work. In the Diabetes Prevention Project trial, diabetes risk reduction was nearly 60% by lifestyle changes and significantly better than metformin or placebo (Figure 2; Knowler et al. NEJM 2002). The second treatment goal is better surveillance of diabetes. Cardiologists should be aware that because of the rising prevalence of diabetes, some heart patients may be undiagnosed. “Before you check the coronary arteries you need to know if that patient has diabetes or not,” said Dr. McGuire. The third treatment goal is to aggressively address the cardiovascular risk that diabetic patients face. The American Diabetes Association recommends the following in order to reduce CVD risk in these patients:
-
Lifestyle counseling including smoking cessation, body weight control, increasing exercise, and improvement in diet
-
Aspirin for those > 40 years of age or those with another cardiac risk factor
-
Use of statins for those > 40 years of age regardless of baseline LDL
-
Blood pressure less than 130/80 mm Hg
-
Ace inhibitors for patients >55 of age with another cardiac risk factor, independent of blood pressure (ADA, 2007)
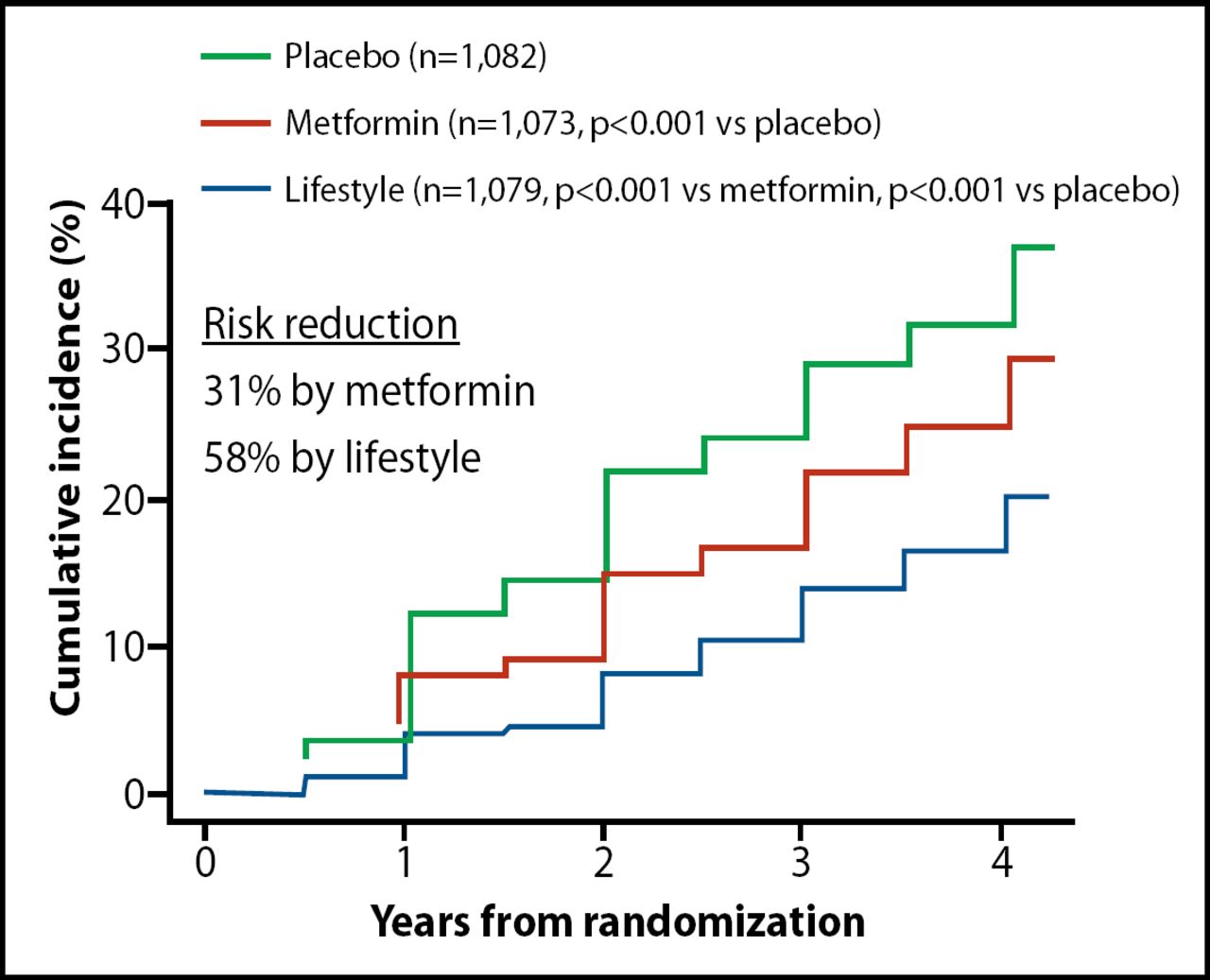
Treatment Goal #1: Preventing Diabetes.
In the face of the epidemics of obesity and diabetes, clinicians should be aware of the problems inherent in these conditions to counsel and treat patients appropriately.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.