

Summary
Quality-of-life and cost-effectiveness analyses of data from patients in the Occluded Artery Trial [OAT] have shown that a strategy of routine percutaneous coronary intervention has modest symptom benefits that diminish over time. The strategy is also more expensive than optimal medical therapy alone.
- cardiology clinical trials
- coronary artery disease
Quality-of-life and cost-effectiveness analyses of data from patients in the Occluded Artery Trial (OAT) have shown that a strategy of routine percutaneous coronary intervention (PCI) has modest symptom benefits that diminish over time. The strategy is also more expensive than optimal medical therapy alone.
In OAT, high-risk asymptomatic patients with a total occluded coronary artery 3–28 days after myocardial infarction (MI) were randomly assigned to either PCI or medical therapy alone and followed for up to 4 years. High-risk was defined as an ejection fraction <50% or proximal occlusion of a main coronary artery. The findings indicated that late opening of the total occluded artery with PCI did not reduce the occurrence of the primary endpoint (a composite of death, nonfatal MI, or heart failure).
Daniel B. Mark, MD, MPH, Duke Clinical Research Institute, Durham, NC, reported the findings of both the quality-of-life and economic analyses. The quality-of-life analysis was carried out on data for 951 patients from the main OAT study. Structured interviews were conducted at baseline (median 6 days post MI) and at 4, 12, and 24 months. The two principal instruments used were the Duke Activity Status Index (DASI) and the SF-36 Mental Health Inventory (MHI); several other quality-of-life instruments were used to determine secondary endpoints.
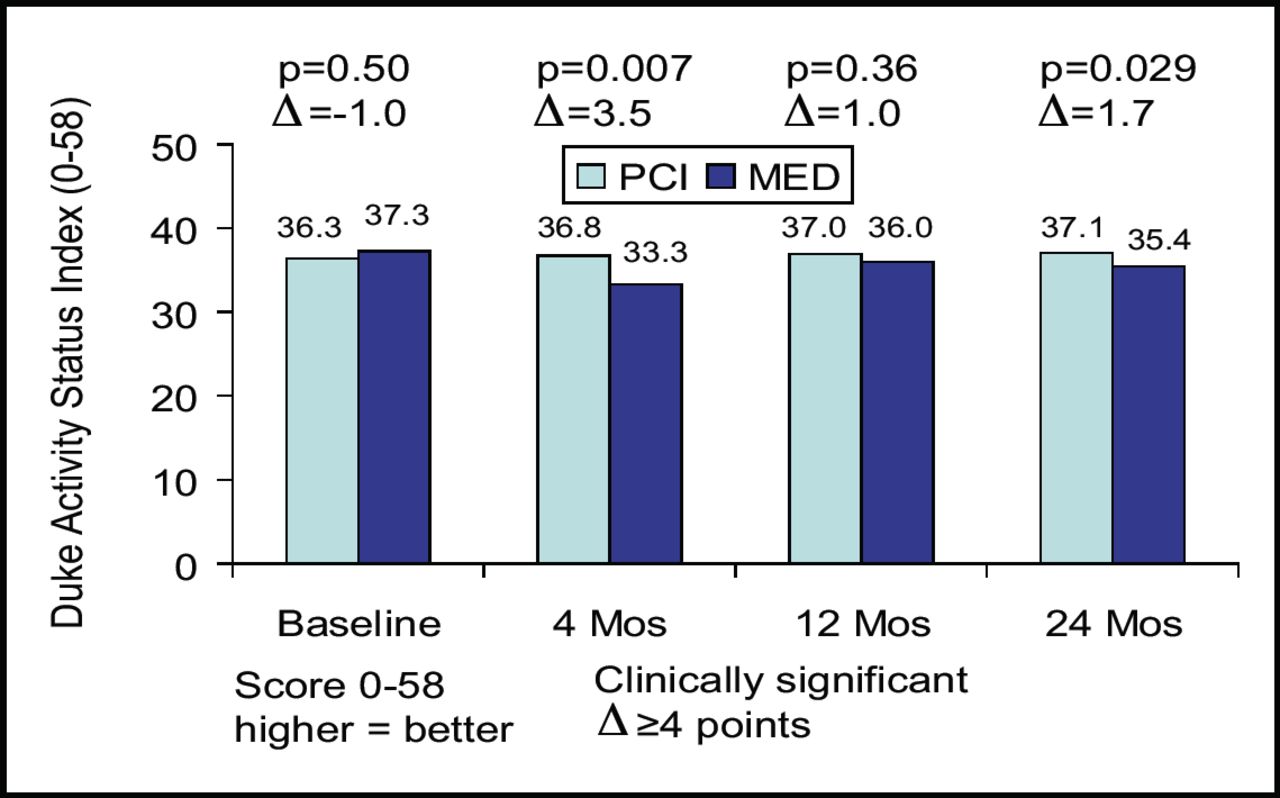
Dr. Mark reported that PCI was associated with a clinically significant benefit in physical functioning at 4 months (p=0.007), according to DASI scores. However, this benefit was not sustained at the 1-year or 2-year follow-up (Figure 1). PCI also had no clinically or statistically significant effect on psychological well-being, according to scores on the SF-36 MHI. Angina on effort decreased over time in both groups, and affected more patients in the medical therapy alone group, but the difference was not significant.
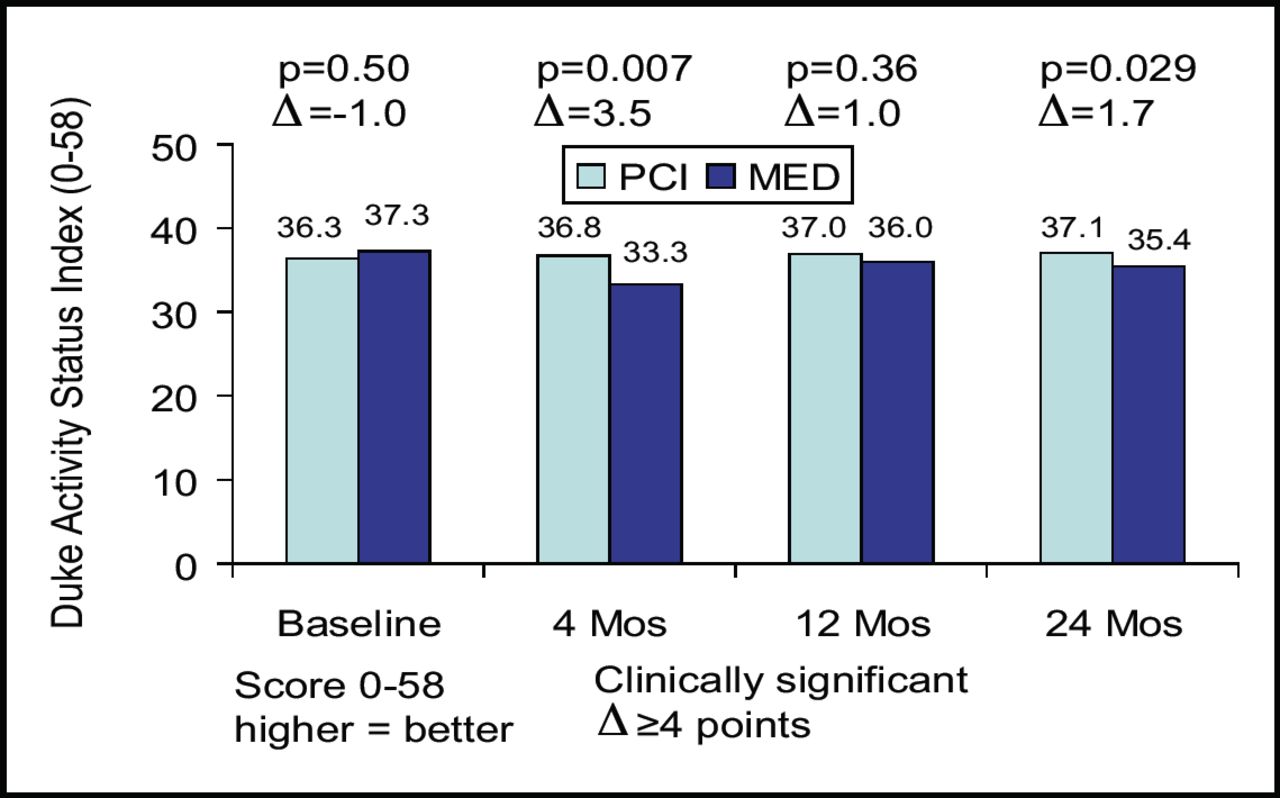
OAT QoL Substudy: Duke Activity Status Index (DASI).
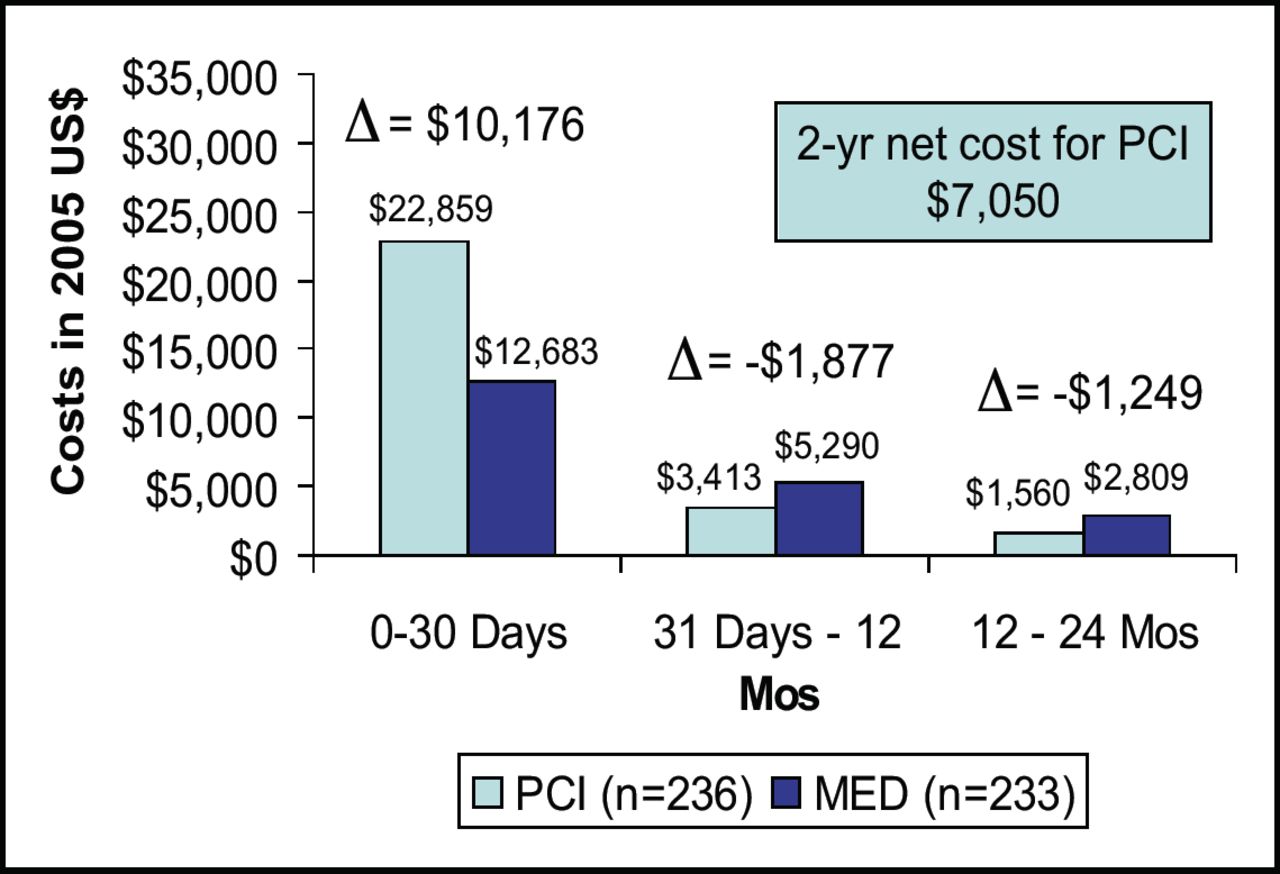
The economic analysis focused on data from 469 patients from the main OAT study who had been treated in US centers. The costs for PCI at 30 days were $10,176 higher than the costs for medical therapy alone; at 1 and 2 years, the costs associated with medical therapy were slightly higher than those associated with PCI. At the end of 2 years, the net excess cost of PCI was slightly over $7,000 (Figure 2).
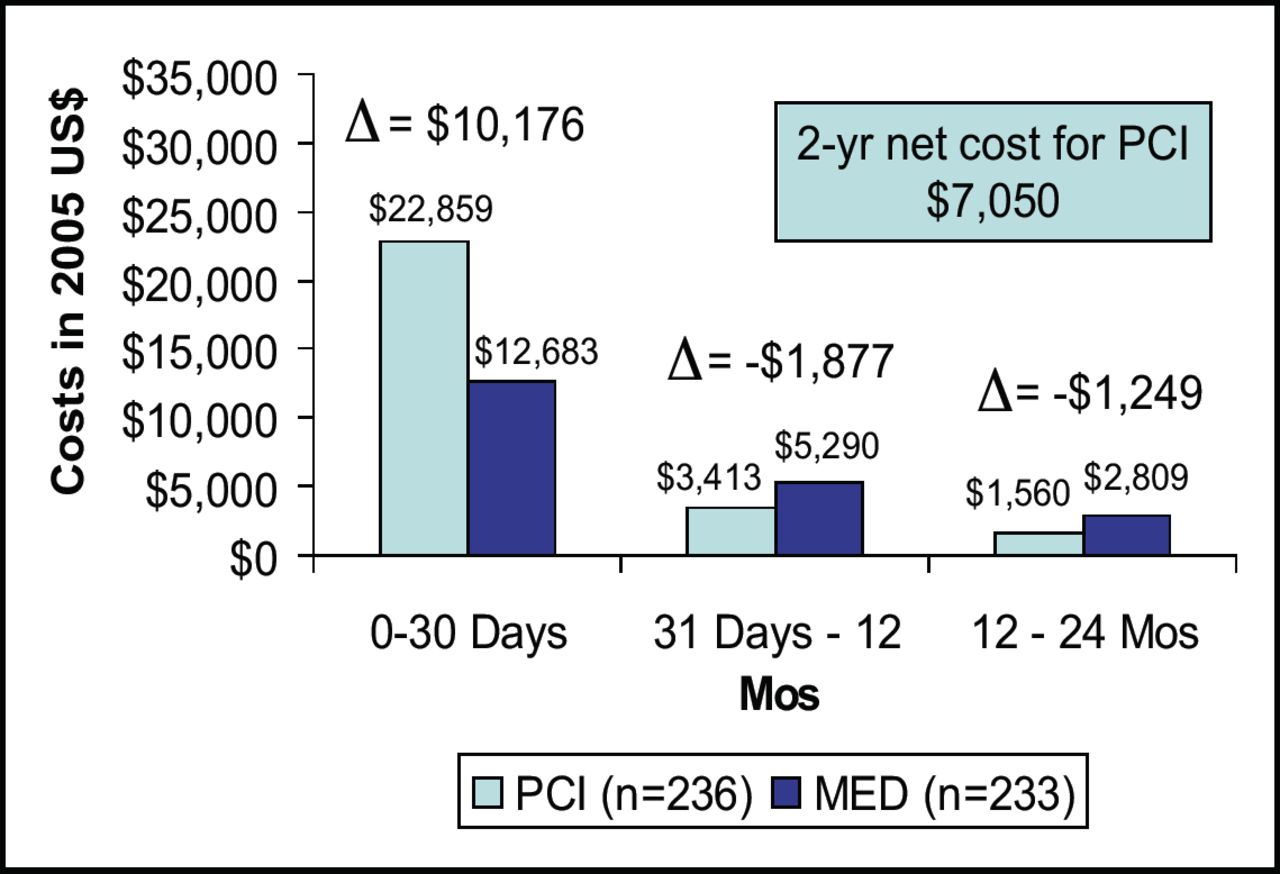
OAT Economic Substudy: Medical (Hosp + MD) Cost in USD by Rx Strategy.
Dr. Mark concluded, “The economic analysis showed that a strategy of routine PCI at 3–38 days after infarction in patients with an occluded infarct artery was substantially more expensive than optimal medical therapy alone out to 2 years and that the small symptom benefit observed was insufficient to make PCI an economically attractive strategy in OAT-eligible patients.”

The editors would like to thank the many members of the AHA 2007 presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.