

Summary
A substudy analysis within the COURAGE trial indicated that percutaneous coronary intervention (PCI) plus optimal medical therapy (OMT) led to significantly improved outcomes in patients with moderate-to-severe ischemia. The substudy results clarify the primary results of the COURAGE trial, reported earlier this year. The main trial results demonstrated that elective PCI plus OMT did not reduce death or MI compared with OMT alone for patients with stable coronary artery disease.
- coronary artery disease clinical trials
- interventional techniques & devices
A substudy analysis within the COURAGE trial indicated that percutaneous coronary intervention (PCI) plus optimal medical therapy (OMT) led to significantly improved outcomes in patients with moderate-to-severe ischemia. According to lead author Leslee Shaw, PhD, Emory University School of Medicine, Atlanta, GA, the substudy results clarify the primary results of the COURAGE trial, reported earlier this year. The main trial results demonstrated that elective PCI plus OMT did not reduce death or MI compared with OMT alone for patients with stable coronary artery disease.
“These findings do not invalidate the earlier results,” said Dr. Shaw. “Rather, they clarify the results and show that there is a differential benefit of PCI in a particular subgroup. The benefit was greatest in patients with more severe ischemia at baseline.”
The substudy involved 314 patients from the main COURAGE population who had rest and stress myocardial perfusion SPECT (MPS) before their assigned treatment and again at 6–18 months after randomization. The primary aim of the study was to compare changes in ischemic burden (defined as a reduction of at least 5% in myocardial ischemia) after an average of 1 year following random assignment to either PCI plus OMT or OMT alone.
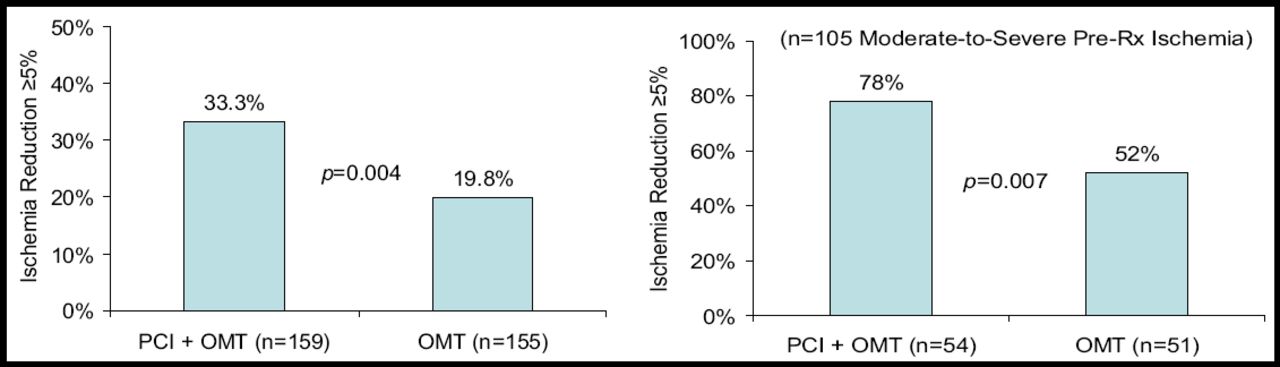
The burden of ischemia at baseline on MPS was similar for both groups (8.2% for PCI plus OMT vs 8.6% for OMT alone). At an average of 1 year, the percentage of patients with a significant reduction (at least 5%) in ischemia (the primary endpoint) was greater for the PCI plus OMT group (33.3% vs 19.8%; p=0.004; Figure 1A). PCI was especially beneficial for patients who had moderate-to-severe ischemia at baseline (perfusion defect ≈10% of myocardium) (78% for the PCI plus OMT group vs 52%; p=0.007; Figure 1B). The mean reduction in ischemic myocardium was also greater in the PCI plus OMT group (−2.7% vs −0.5% for OMT alone; p<0.0001).
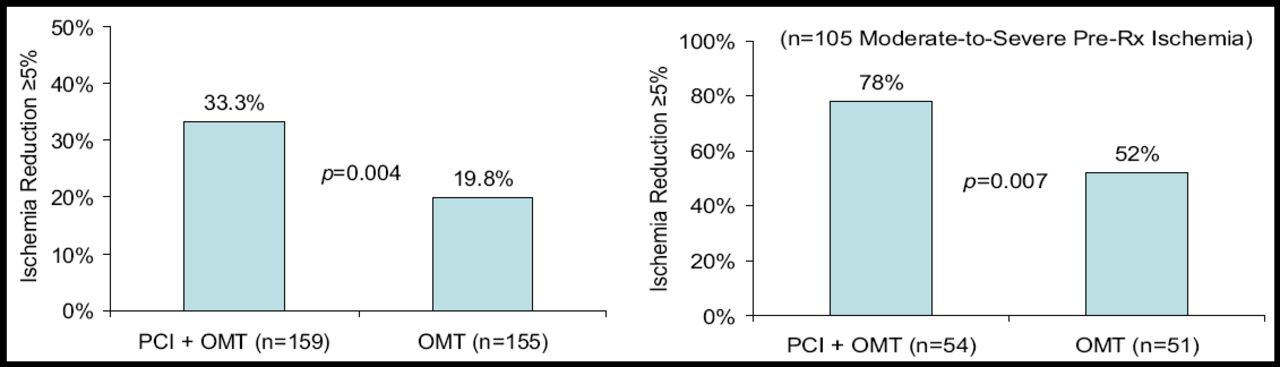
Primary Endpoint: % with Ischemia Reduction ≥5% Myocardium (n=314) and % with Ischemia Reduction ≥5% Myocardium.
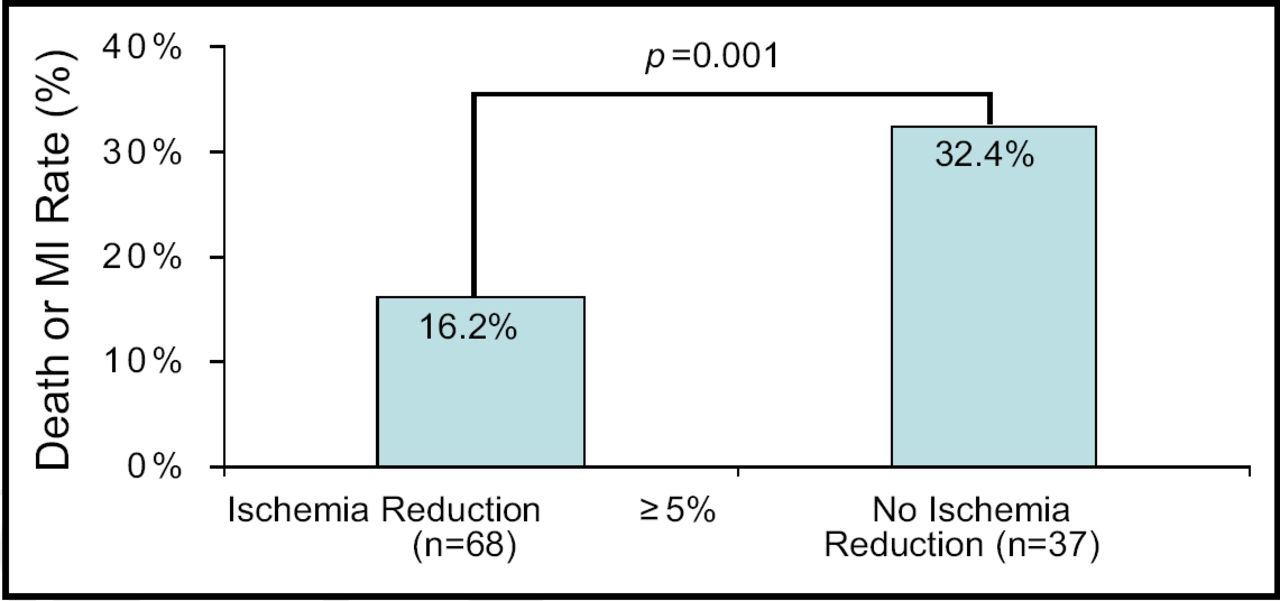
In addition, in an attempt to correlate the extent of myocardial ischemia to clinical outcomes, Dr. Shaw showed that the risk of death or MI was lower among patients who had a reduction in ischemia of at least 5% (13.4% vs 24.7%; p=0.037), particularly among patients with moderate-to-severe ischemia before treatment (16.2% vs 32.4%; p=0.001; Figure 2). The rates of death and MI ranged from 0–39% according to the amount of residual ischemia after PCI.
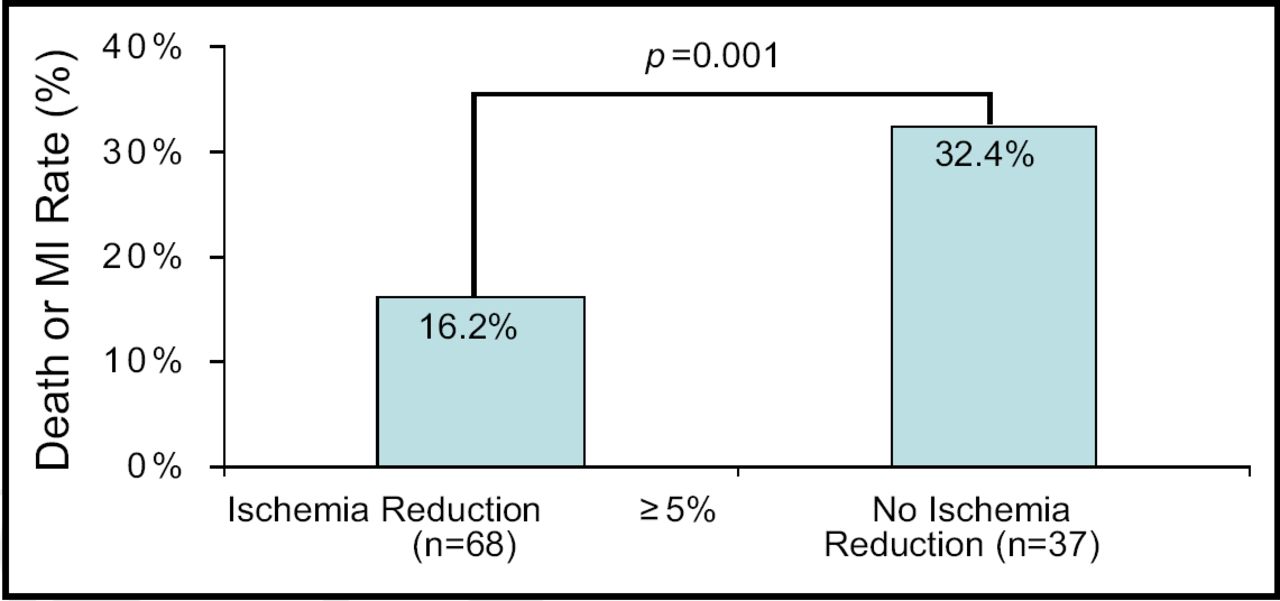
Risk of Death or MI Among Patients with Moderate-to-Severe Ischemia.
Dr. Shaw emphasized that although the findings suggest that MPS may be valuable for identifying patients at risk for death or MI, the prognostic findings in this substudy were exploratory with limited statistical power. Still, she said, “These findings suggest the potential value of MPS in identifying at-risk patients for targeting therapy and in guiding treatment strategies, particularly for patients with moderate-to-severe pre-treatment ischemia who may benefit with PCI as well as consideration of crossover to PCI for those patients with extensive residual ischemia following a course of medical management.”
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.