

Summary
This article presents the results of the Resynchronization Therapy in Normal QRS [RethinQ] study. This study was conducted in patients with New York Heart Association Class III congestive heart failure, left ventricular ejection fraction = 35%, narrow QRS (<130 ms), and evidence of mechanical dyssynchrony via echocardiography, who were candidates for an implantable cardioverter defibrillator.
- cardiology clinical trials
- interventional techniques & devices
- heart failure
John F. Beshai, MD, University of Illinois-Chicago, presented the results of the Resynchronization Therapy in Normal QRS (RethinQ) study. This study was conducted in patients with New York Heart Association (NYHA) Class III congestive heart failure (CHF), left ventricular ejection fraction ≤ 35%, narrow QRS (<130 ms), and evidence of mechanical dyssynchrony via echocardiography, who were candidates for an implantable cardioverter defibrillator (ICD). Patients with permanent atrial fibrillation, prior cardiac resynchronization therapy (CRT), unstable angina, recent myocardial infarction, or revascularization were excluded. The primary goal of the study was to determine the efficacy of CRT in these patients as measured by an improvement in peak VO2 testing (>1.0 mL/kg/min) during cardiopulmonary exercise stress at 6 months. A total of 85 patients were randomized to receive an ICD and optimal medical therapy (control group) and 87 patients received an ICD, CRT, and optimal medical therapy (CRT group); 156 patients were included in the efficacy dataset. Patients were stratified by QRS greater than or less than 120 ms and whether or not they had ischemic or non-ischemic cardiomyopathy. All patients were followed for 6 months.
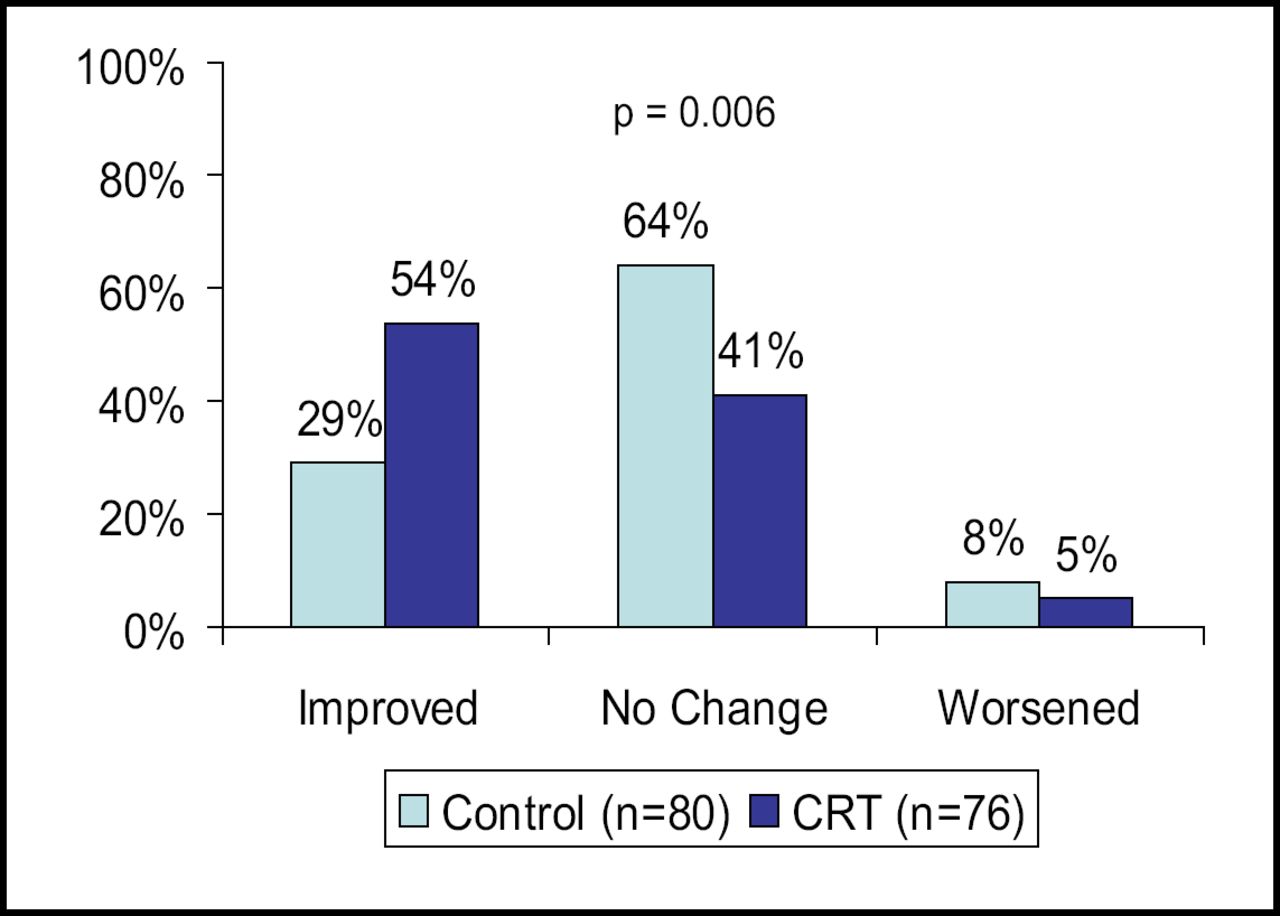
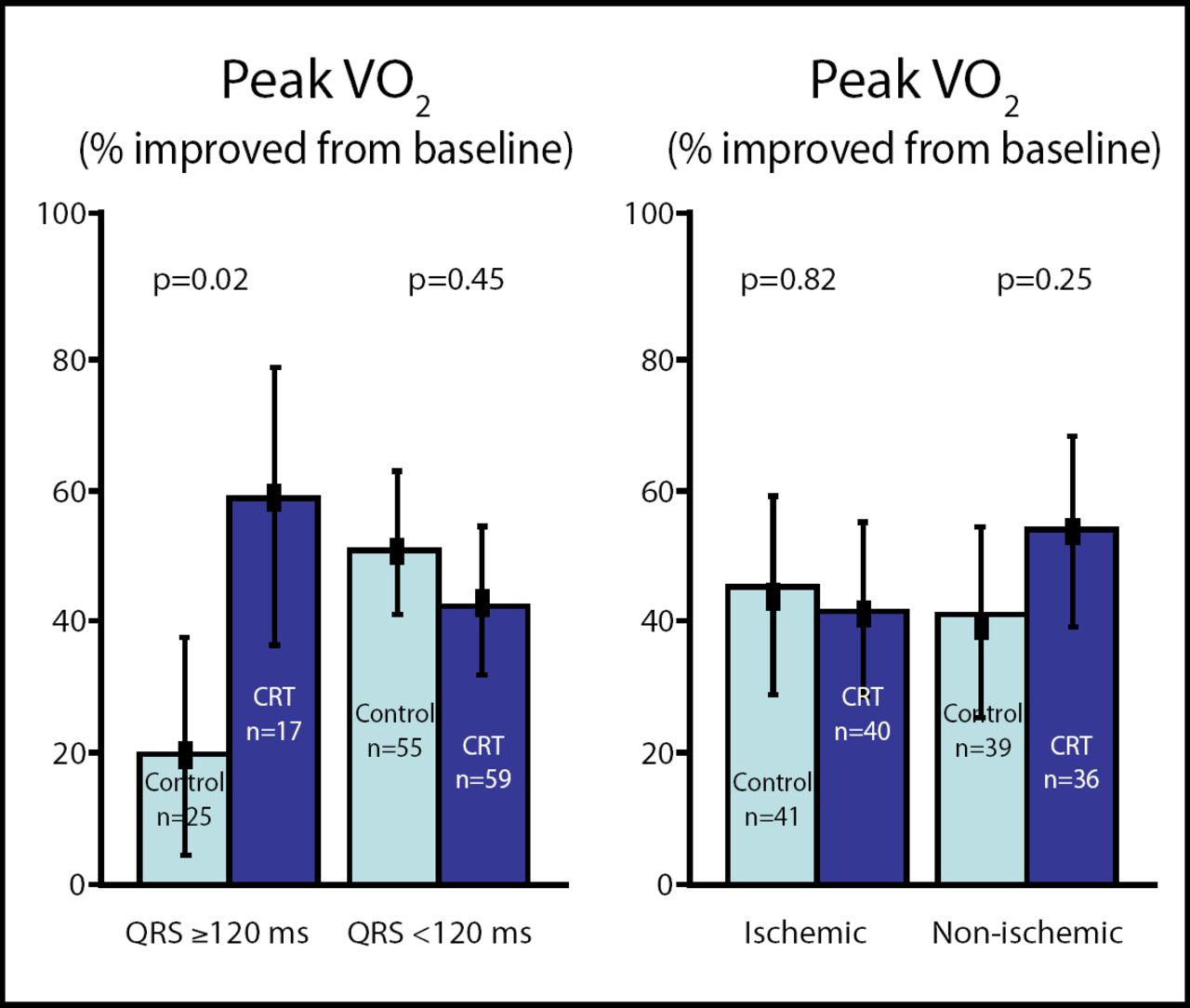
The mean age of the participants was 58 years in the control group and 62 in the CRT group. The mean QRS values in the control and CRT groups were 106 ms and 107 ms, respectively, and approximately one-half of the participants in each group had ischemic cardiomyopathy. The majority of the patients was male (58% control and 71% CRT, respectively). The study did not meet its primary endpoint, with 46% of CRT patients experiencing improvement in peak VO2 versus 41% in the control group (p=0.63). There were no significant differences between treatment groups in quality of life measures or left ventricular volumes and dimensions. The CRT group had a significant improvement in the secondary measure of NYHA class when compared with the control group (p=0.006; Figure 1). Additionally, subgroup analyses indicated a significant improvement in CRT patients with a QRS duration between 120 and 130 ms (p=0.02), but there were no significant differences based on the presence or absence of ischemia (Figure 2).
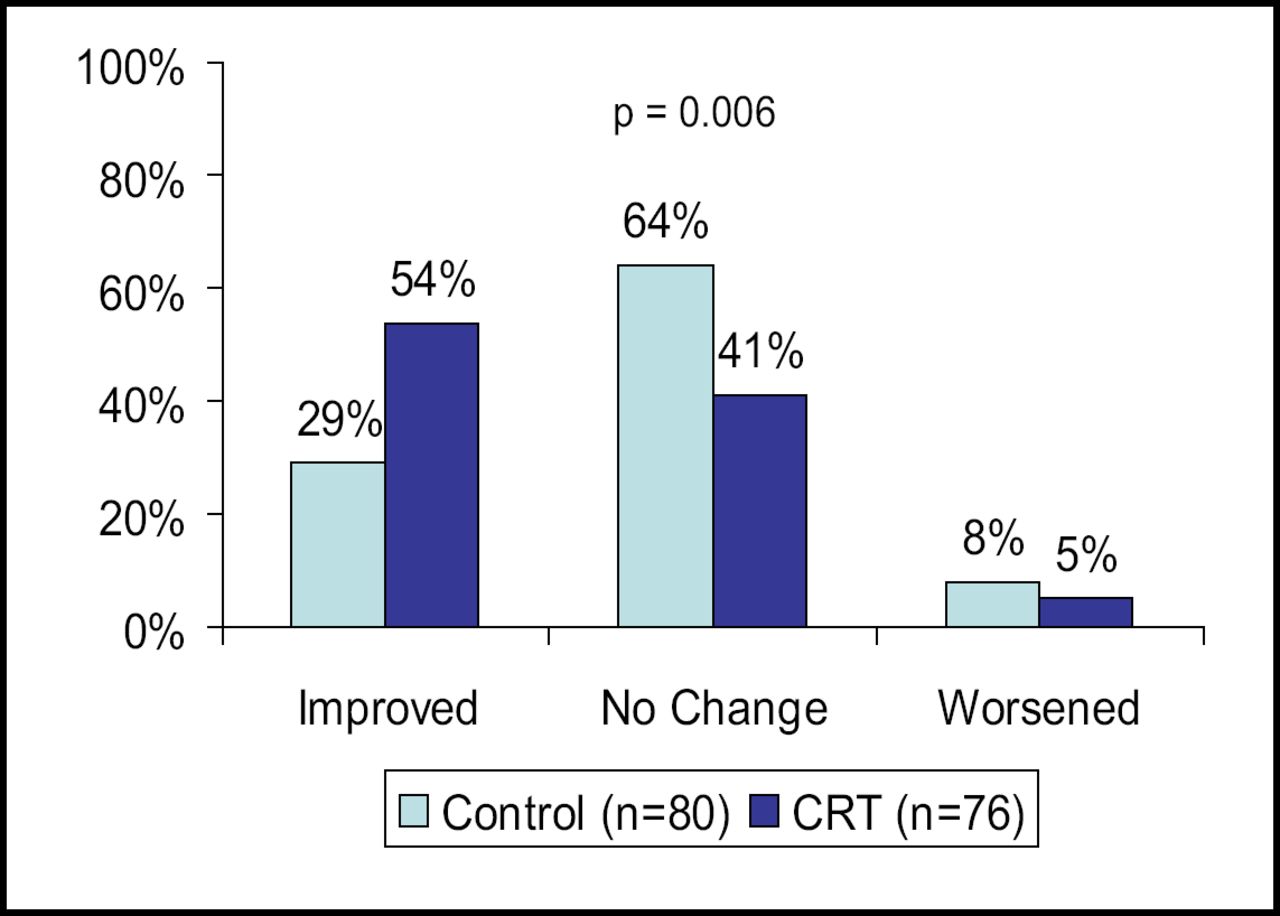
NYHA Class.
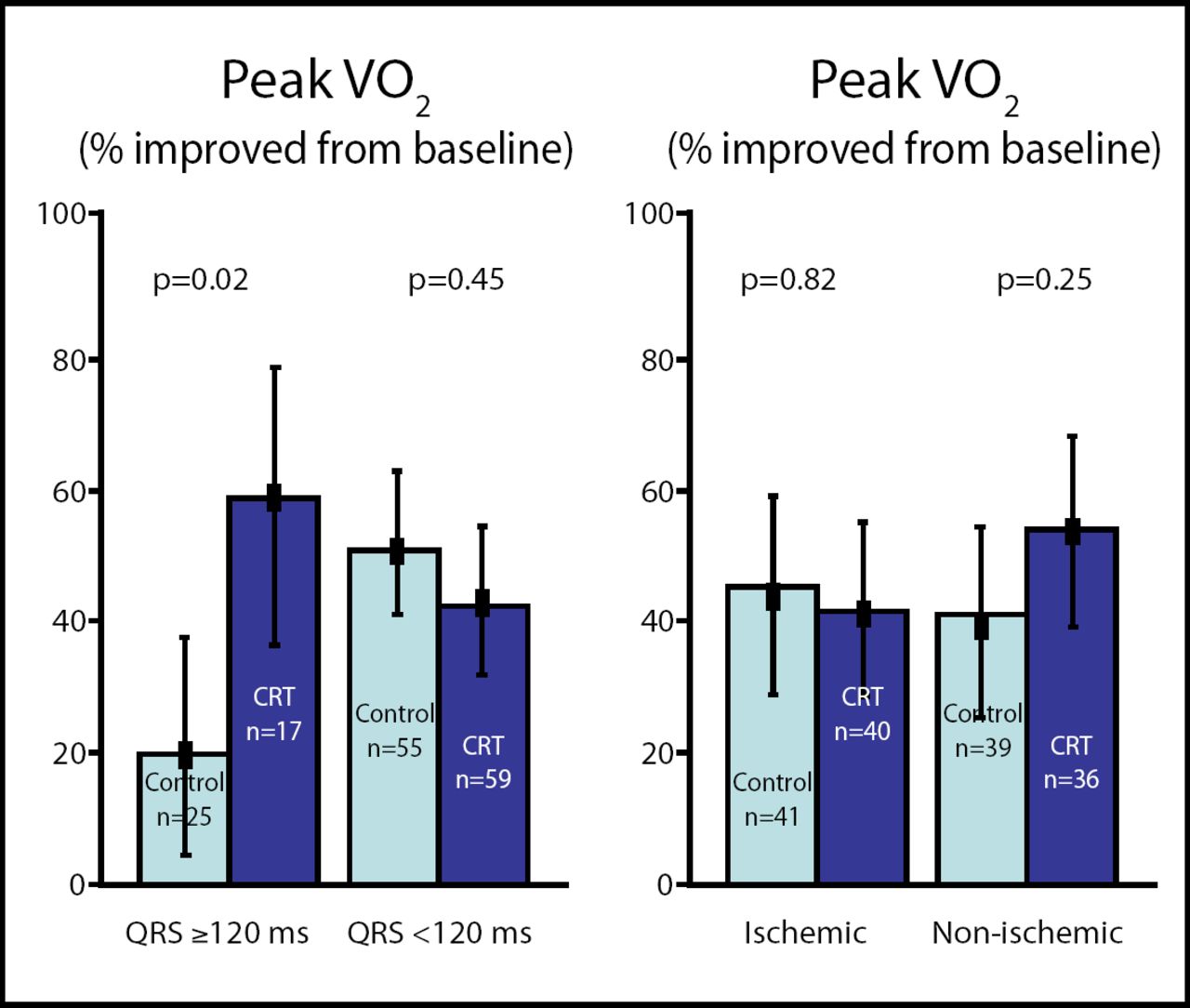
Peak VO2 by Subgroup.
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
“Additional research will be critical to further our understanding of the role of CRT in this patient population”, summarized Dr. Beshai.
The findings of this study have been published: [Beshai et al. NEJM. 357(24):2461–71].
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.