

Summary
The relationship between plasma triglycerides and low-density lipoprotein cholesterol (LDL-C) appears to be parabolic rather than linear. This finding suggests that apolipoprotein B may be superior to LDL-C as a marker for cardiovascular disease risk.
- diabetes & endocrinology clinical trials
- diabetes mellitus
- lipid disorders
The relationship between plasma triglycerides and low-density lipoprotein cholesterol (LDL-C) appears to be parabolic rather than linear. The finding, stated investigator Martijn C.G.J. Brouwers, MD, Cardiovascular Research Institute Maastricht, the Netherlands, suggests that apolipoprotein B (apo B) may be superior to LDL-C as a marker for cardiovascular disease risk.
Elevated LDL-C along with elevated plasma triglycerides and decreased HDL-cholesterol in the presence of small dense LDL is known to strongly increase cardiovascular risk. The latter three lipid derangements are frequently found in the metabolic syndrome, familial combined hyperlipidemia, and type 2 diabetes. What has not been clear, however, stated Dr. Brouwers, is why LDL-C is often “fairly normal” in patients with type 2 diabetes, while triglycerides are moderately elevated.
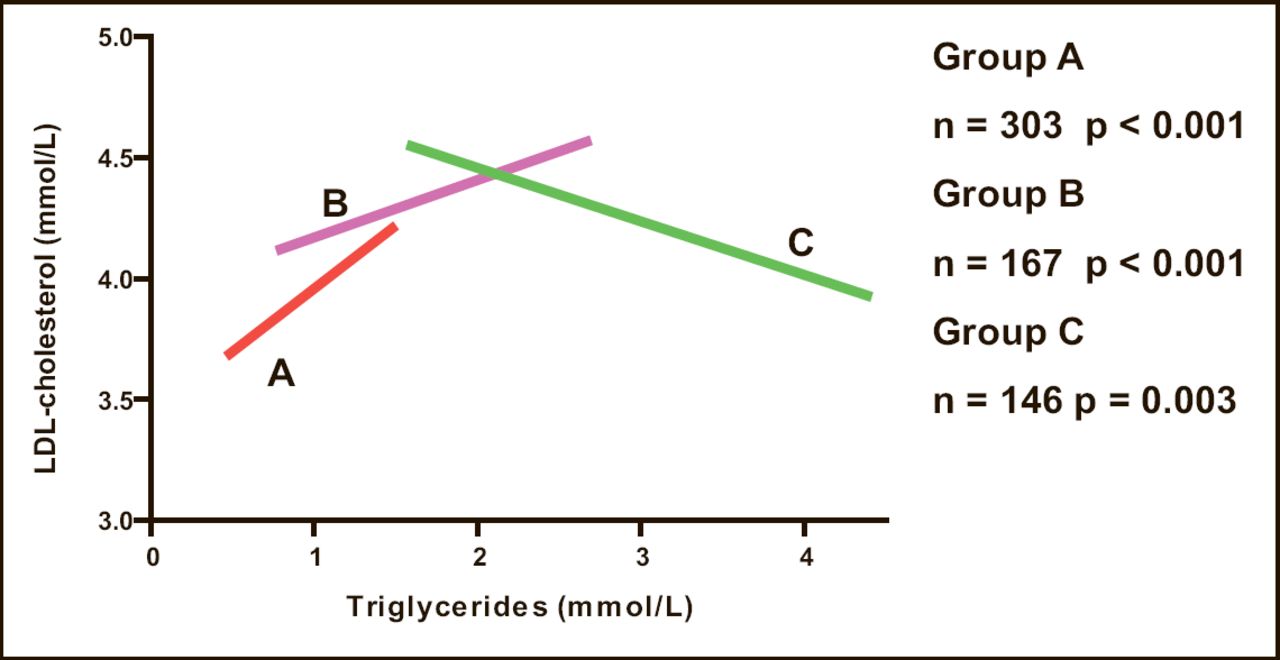
Dr. Brouwers and colleagues speculated that the relationship could be parabolic, such that at low triglyceride levels (<1.5 mmol/L) an increase in plasma triglycerides is accompanied by an increase in LDL-C, whereas a further increase in triglycerides is followed by a decline in LDL-C. To test the hypothesis they analyzed 6-year data from the Hoorn Study which contains data from the general Dutch population. Patients (n=1,343; aged 50–75 years) were stratified into three groups based on plasma triglyceride levels obtained twice over 6 years: Group A: <1.5 mmol/L at both time points; Group B: one measurement below and one above 1.5 mmol/L; and Group C with both measurements >1.5 mmol/L.
The results showed that in Group A and Group B males, the relationship between plasma triglycerides and LDL-C was positive (p<0.001 for both). For Group C males, the relationship was negative (p<0.003; Figure 1). The same pattern was found among women, but the negative relationship did not attain statistical significance (p=0.4). Across all groups, the results did not differ among patients with and without diabetes. An analysis among men with familial combined hyperlipidemia revealed a similar pattern with statistically significant positive and negative relationships for Group A (p<0.001) and Group C (p=0.002).

General Population (Men).
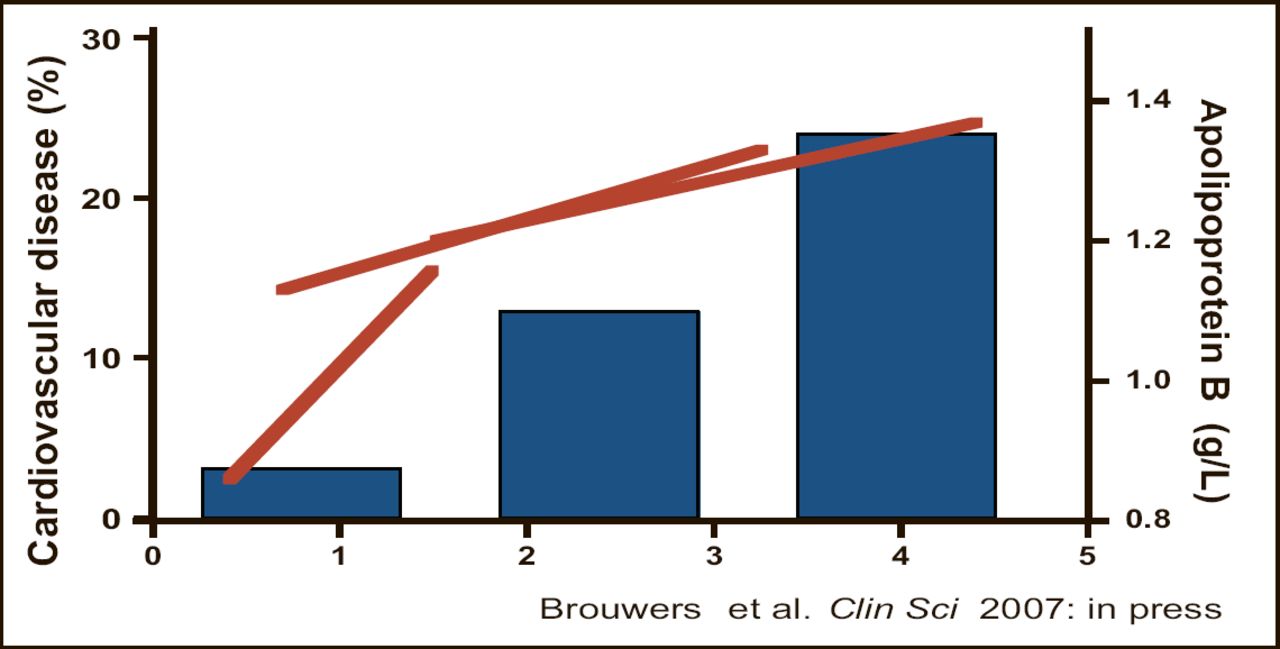
Of interest, a more linear relation was observed between plasma triglycerides and apo B levels and the prevalence of cardiovascular disease (Figure 2).

Familial Combined Hyperlipidemia (Men).
The existence of a parabolic (vs linear) relationship between triglycerides and LDL-C provides more insight into the complex relationships of clinically relevant cardiovascular risk factors and shows that one cannot be interpreted without the other Dr. Brouwers concluded.
In an interview, he commented that cardiologists should not trust measuring only LDL-C levels because that measure reveals information about both the quantity and quality of lipid particles – which can be confusing. Specifically, low LDL-C levels can indicate reduced particle number, which would be favorable for cardiovascular risk, or reduced particle size, which would be unfavorable. Looking at triglycerides or HDL-C, which are both indicative of LDL quality, combined with apo B might be a better strategy, he suggested. “Remember, every lipid particle contains one apo B molecule, so higher levels mean higher risk.” He said further that when triglycerides are high and HDL is low, LDL-particles will be small and atherogenic. He cautioned, however, that apo B measurement techniques vary widely and that standardization and further studies are needed before a risk calculator based on apo B can be derived.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.