

Summary
A study of Dutch subjects [Cohen D et al. Diabetes Care 2006] found previously undiagnosed diabetes in 14.5% of subjects with severe mental illness versus 1.5% in the general population. This and other studies have also found a high frequency of impaired glucose tolerance among the severely mentally ill. This article discusses the role of antipsychotic drugs, the management of metabolic issues in psychiatric patients, and diabetes and depression.
- diabetes mellitus
- cardiometabolic disorder
- mood disorders
- schizophrenia
A recent study of Dutch subjects [Cohen D et al. Diabetes Care 2006] found previously undiagnosed diabetes in 14.5% of subjects with severe mental illness versus 1.5% in the general population. This and other studies have also found a high frequency of impaired glucose tolerance among the severely mentally ill.
This association is likely multifactorial and involves not only antipsychotic agents but also unhealthy lifestyles and genetics. A family history of type 2 diabetes has been found in up to 30% of patients with schizophrenia. Regions of the human genome that overlap diabetes and schizophrenia have also been identified, as well as overlaps in the regulatory enzymes for glycolysis and schizophrenia. It has also been shown that beta-cell function and insulin resistance improve as psychosis improves [Shiloah E et al. Diabetes Care 2003].
Jogin H. Thakore, PhD, St. Vincent's Hospital, Dublin, Ireland, discussed possible mechanisms for these associations. He reported that patients having a first episode of schizophrenia have three times as much intra-abdominal fat as matched controls and that impaired glucose tolerance is found in 15% of patients with schizophrenia and in 18% of their first-degree relatives. These patients also have increased expression of a surface-bound platelet glycoprotein that is critical for platelet aggregation. “This may partly explain the increased predisposition of the severe mentally ill to cardiac events,” Dr. Thakore suggested.
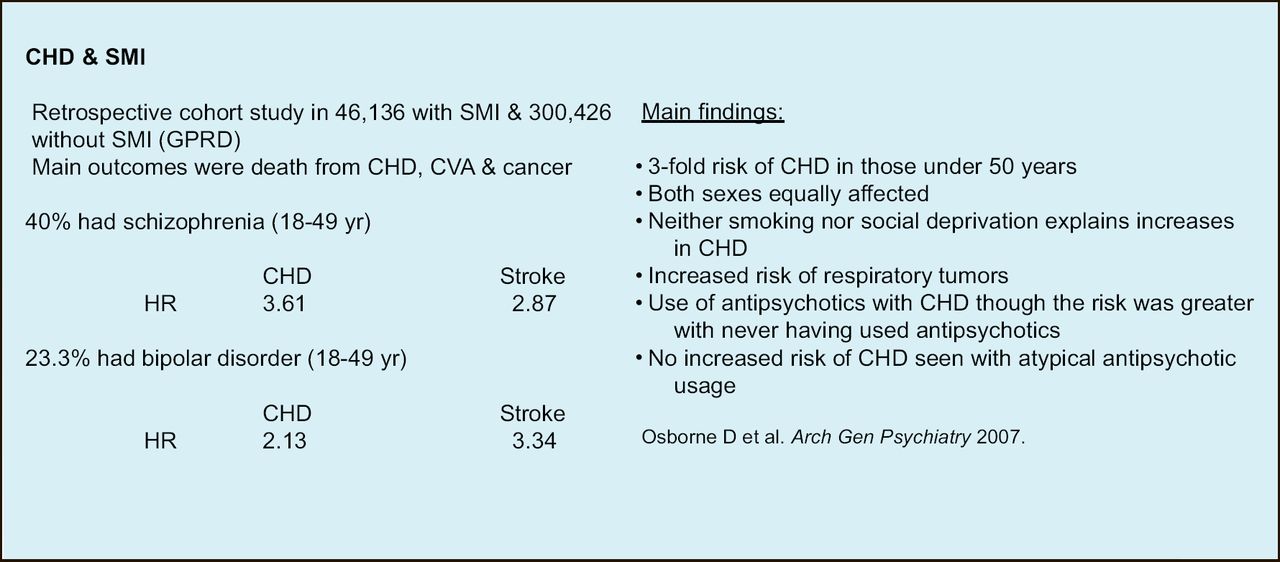
Coronary heart disease is now the leading cause of death among persons with severe mental illness (Figure 1) [Osborn DP et al. Arch Gen Psychiatry 2007] suggesting that persons with schizophrenia and their relatives may benefit from cardiovascular screening.

Rates of Coronary Heart Disease in Patients with Severe Mental Illness.
Role of Antipsychotic Drugs
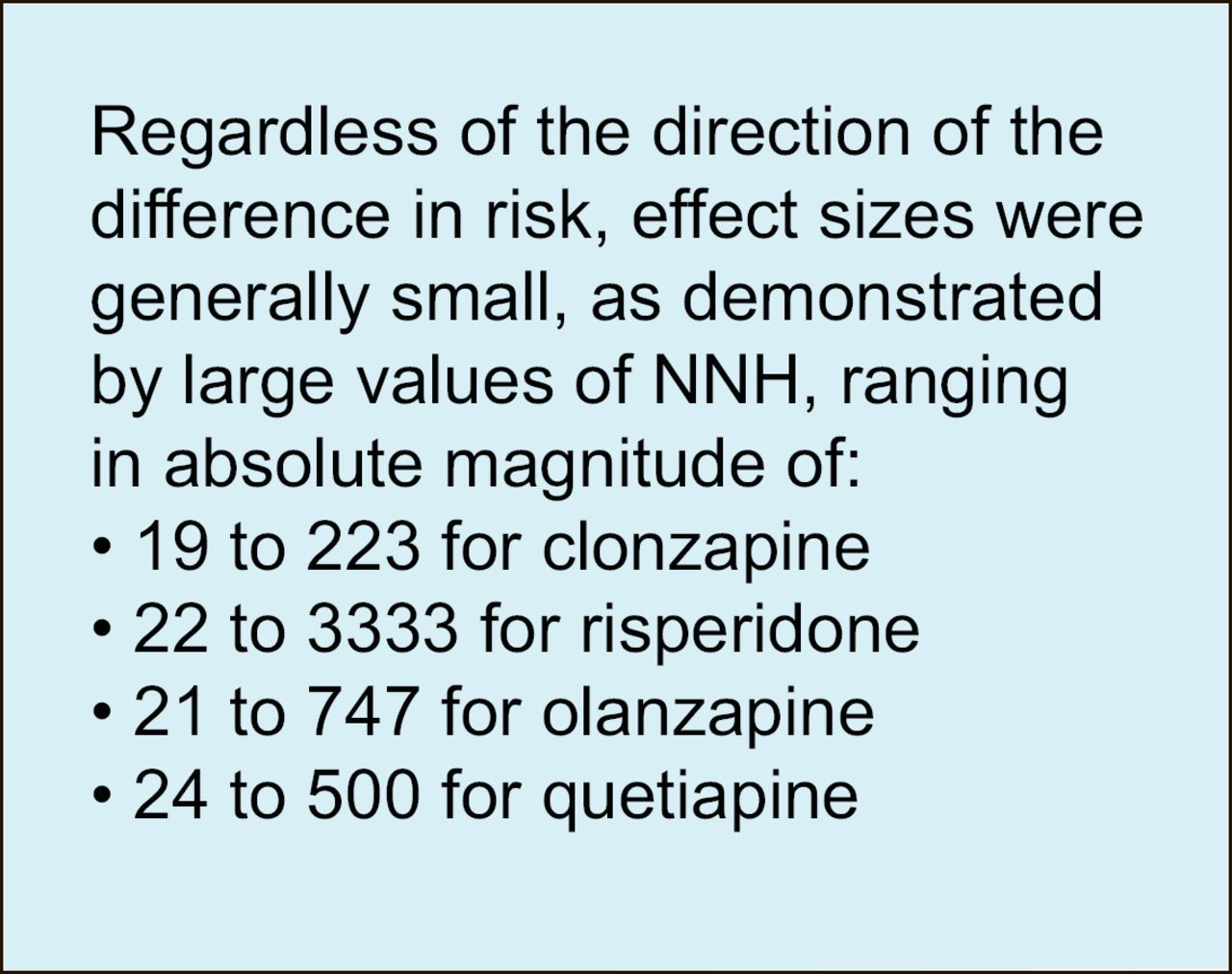
Type 2 diabetes has been reported to develop during treatment for schizophrenia. The role of second-generation antipsychotic agents in worsening glucose tolerance has been actively explored. Leslie Citrome, MD, New York University School of Medicine, New York, United States, presented the results of a recent study that showed that the second-generation antipsychotics were associated with a range of 53 more cases of diabetes to 46 fewer cases of diabetes per 1,000 patients (Figure 2) [Citrome LL et al. Ann Pharmacother 2007].

Risk of Diabetes Attributable to First- and Second-Generation Antipsychotic Agents.
“There was little observable difference between individual second-generation antipsychotics versus first-generation antipsychotics” Dr. Citrome said. Few studies, however, controlled for confounding factors such as body weight, family history and physical activity, he added. “Prolonged exposure to an individual agent can cause problems, though the attributable risk remains unknown. The choice of antipsychotic cannot predict who will develop type 2 diabetes.” Differences among the antipsychotics regarding weight gain and lipid alterations must be balanced with the need to provide for more efficacious psychiatric treatment, he said.
Practical Management of Metabolic Issues in Psychiatric Patients
Persons with severe mental illness have triple the mortality rate of the general population and die 10–20 years earlier. For 33- 60%, death is due to cardiovascular disease. An increased prevalence of diabetes and the metabolic syndrome may explain this, said Richard Holt, MD, University of Southampton, UK.
The Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study found that over 85% of schizophrenic patients had at least one feature of the metabolic syndrome [McEvoy JP et al. Schizophr Res 2005]. “The management of metabolic predictors in patients with severe mental illness is a neglected area,” Dr. Holt said. “You should consider this problem from the first day a patient is diagnosed with mental illness.”
Dr. Holt recommended that patients should be screened for the metabolic syndrome and cardiovascular risk prior to starting antipsychotic therapy. They should undergo a fasting blood glucose test, or at least a random blood glucose screen. After 3–4 months of treatment, the test should be repeated to identify treatment-emergent diabetes, and then repeated annually. Standard risk factors should be assessed annually and treated. Dr. Holt said that he had been successful with lifestyle intervention programs in people with mental illness.
“Just reliably measuring cardiovascular risk factors and treating these patients as you would treat the general public would be a great leap forward,” he said.
Certainly, there are special issues in managing this patient population. “These patients are challenging at best,” he observed. There should be liaisons between the diabetes and psychiatric services. Most importantly, adequate mental treatment should be maintained and the antipsychotic drug should only be stopped if it is the major cause of the diabetes.
Diabetes and Depression
Diabetes is also associated with other mental illness. Major depressive disorder occurs in 10% of diabetics, and subclinical symptoms occur in another 10–40%. For reasons that are unclear, depression also increases the odds of developing type 2 diabetes, and when both conditions are present, diabetic outcomes are worsened, said Patrick J. Lustman, MD, Washington University, St. Louis, Missouri, United States.
Depression also seems to increase the risk of developing diabetes. In the prospective Stockholm Diabetes Prevention Program which comprised 5,500 subjects, men (although not women) with the highest level of depressive symptoms had a nearly four-fold risk for type 2 diabetes and a nearly two-fold risk for a prediabetic state, compared with the least depressed, reported Claes-Göran Östenson, MD, Karolinska Institute, Stockholm, Sweden.
Depressed patients actually have an increased risk for virtually all factors of the metabolic syndrome except hyperlipidemia. Compared to non-depressed diabetic patients, patients who have both diabetes and depression have poorer glycemic control, a higher risk of multiple morbidities and mortality, increased functional impairment, and poorer adherence to diet, exercise and self-management strategies, said Professor Norbert Hermanns, Research Institute of the Diabetes Academy Mergentheim, Bad Mergentheim, Germany.
Frans Pouwer, PhD, VU Medical Center, Amsterdam, the Netherlands, added that all of the complications of diabetes are associated with increased scores on depression instruments, most likely because of “the hardship and chronic stress” of having diabetes and its complications. He pointed to the results of a recent study that showed that persons with type 1 or type 2 diabetes were more likely to have attempted suicide than the general Dutch population (6.4% vs 2.7%). Those with previous suicide attempts tended to have higher HbA1c levels, more diabetic complications, and more erectile dysfunction. Not surprisingly, 94% of these subjects scored high on measures of depression, compared with 24% of non-suicidal diabetic subjects [Pouwer F et al. EASD 2007].
In another report, Mirjana Pibernik-Okanovic, PhD, Vuk Vrhovac University Clinic, Zagreb, Croatia, examined patterns of glycemic control in “emotionally burdened” subgroups versus symptom-free individuals. The study of 470 type 2 diabetics found that 44% had severe depressive symptoms, high levels of “diabetes-related distress,” or the combination of symptoms. Depressive symptoms combined with diabetes-related distress most adversely affected glycemic control. These levels improved at 1 year in the “distressed” group but not in the depressed groups.
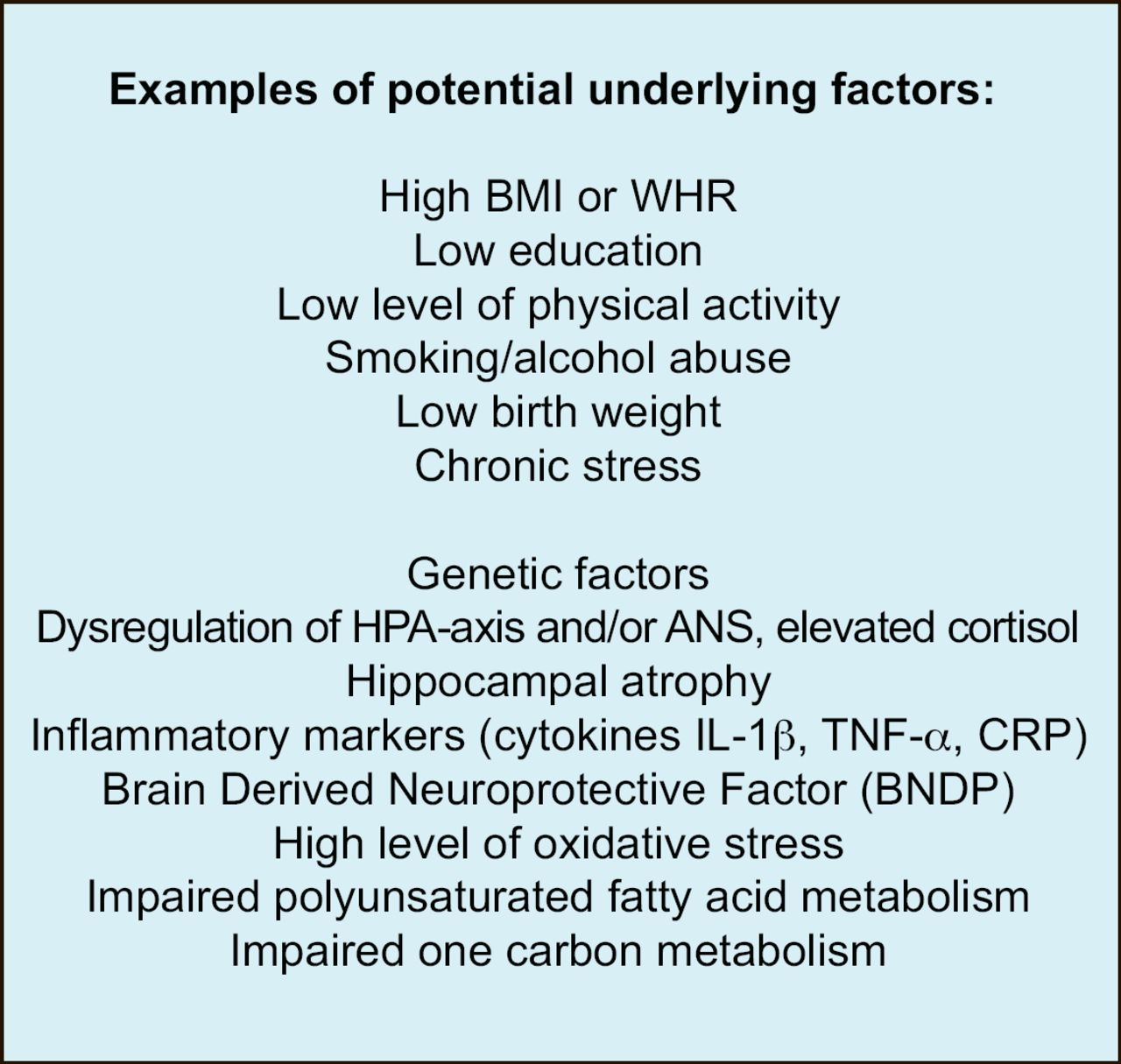
Behaviors that accompany depression may be partly to blame for such adverse outcomes, Prof. Pouwer said, noting that depressed patients are less likely to adhere to diet, exercise, and glucose self-monitoring. There are also numerous biochemical factors linking impaired glucose metabolism with depression, especially those related to the human stress response (Figure 3), he added.

Factors Underlying Poor Glycemic Control in Depressed Patients.
“Depression in diabetes has to be taken seriously,” emphasized Prof. Hermanns. Recent results of the World Health Survey [Moussavi S et al. Lancet 2007] show that combination of diabetes and depression has the most negative impact on health among a dozen or so serious medical conditions. Unfortunately, studies show that depression remains undetected and thus untreated in 50–75% of diabetics who have it.
Adequate treatment of depression seems to impact the prognosis of diabetes as well. Dr. Lustman and colleagues have shown that treatment with the dual norepinephrine and dopamine reuptake inhibitor bupropion not only improves depression but also improves glycemic control. The same may be true with the selective serotonin reuptake inhibitors, but not with nortriptyline, a norepinephrine reuptake inhibitor [Lustman PJ et al. Diabetes Care 2007].
Richard Rubin, PhD, Johns Hopkins University, Maryland, United States, encouraged the use of antidepressant medications in diabetic patients, but said that counseling, especially cognitive behavioral therapy, is also important for patients with poorly controlled glycemia. Since depression often recurs, careful monitoring is important with some patients requiring chronic long-term treatment.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.