

Summary
It is now well established that cardiovascular disease is the most common cause of death among diabetics, and that diabetes is an independent risk factor for cardiovascular events. The effect of diabetes on the heart however, is not limited to the vasculature and can extend to the myocardium as well as in the form of diabetic cardiomyopathy. The associations between diabetes and damage to the heart and vascular system are not fully understood.
- diabetes mellitus
- inflammatory disease
It is now well established that cardiovascular disease is the most common cause of death among diabetics, and that diabetes is an independent risk factor for cardiovascular events. The effect of diabetes on the heart however, is not limited to the vasculature and can extend to the myocardium as well as in the form of diabetic cardiomyopathy. The associations between diabetes and damage to the heart and vascular system are not fully understood.
Diabetic Cardiomyopathy
“Does ‘diabetic cardiomyopathy’ really exist?” asked Paul Poirier, MD, Hospital Laval, Quebec. Based on clinical and experimental lines of evidence, the answer is “yes.” Sustained diabetes leads to deterioration of cardiac function independent of macro-and microvascular disease. “Because heart disease is the major cause of mortality in patients with diabetes, early detection of altered cardiac function is important to improve medical interventions and outcomes,” he emphasized.
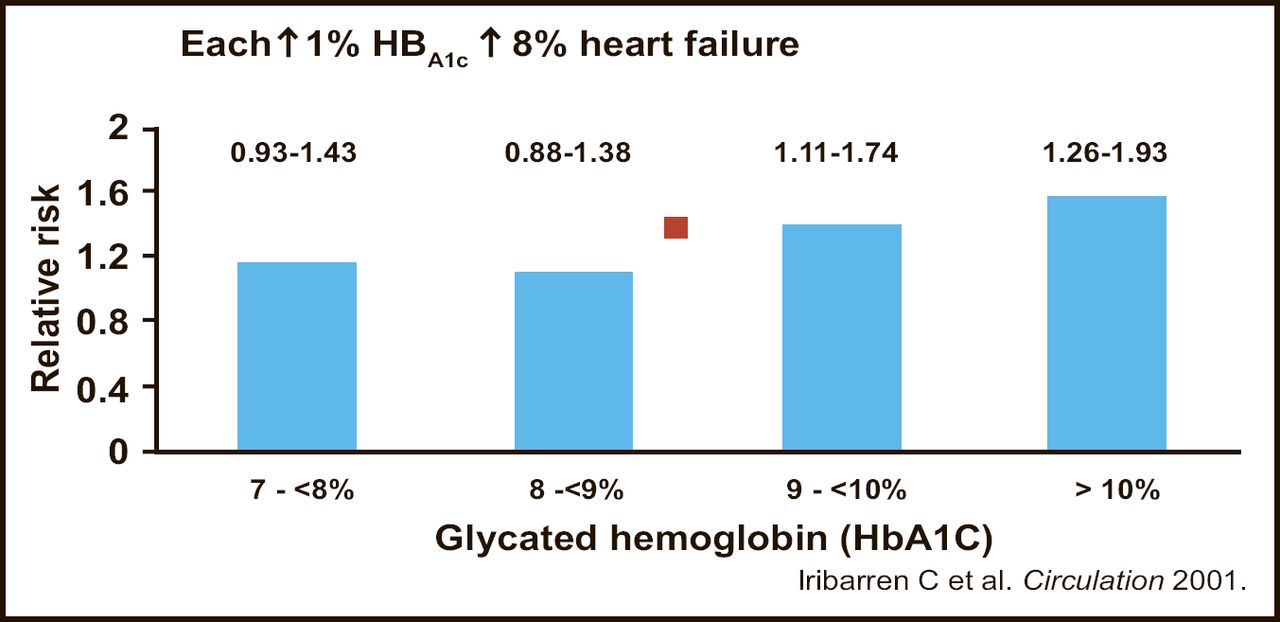
Idiopathic cardiomyopathy is 9 times more frequent among diabetics than among non-diabetic subjects, according to a case control study of 500,000 hospitalized patients [Bertoni AG et al. Diabetes Care 2003]. It occurs in both type 1 and type 2 diabetes, and appears to be related to glycosylated hemoglobin. One study found that for each 1% increase in HbA1c levels, there was an 8% increase in the incidence of heart failure [Iribarren C et al. Circulation 2001] (Figure 1). Independent risk factors for heart failure included increased age, longer duration of diabetes, use of insulin, and increased body weight.

Diabetes and Heart Failure.
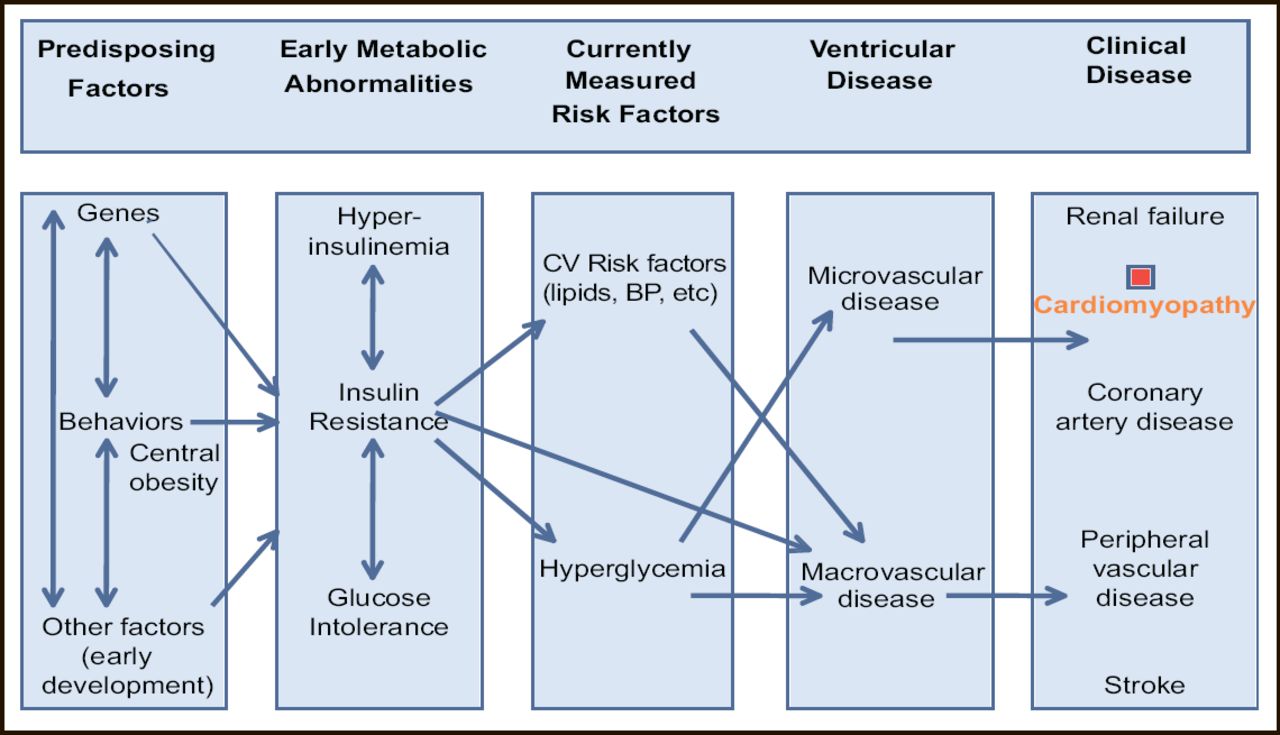
“But diabetic cardiomyopathy is an ill-defined entity,” Prof. Poirier continued. Clinically, diabetic cardiomyopathy cannot be distinguished from other forms of heart failure in diabetic patients. The scenario of diabetic cardiomyopathy includes early impairment of diastolic function (possibly the earliest clinical sign), subclinical abnormal cardiac metabolism, and cardiac autonomic neuropathy. “Early on, the preclinical manifestations may not seem significant in daily life,” he said. With further injury to the abnormal myocardium, systolic dysfunction occurs years later (Figure 2).

Diabetic Cardiomyopathy.
The worse the diastolic dysfunction, the lower the energy efficiency of the heart. Patients with diabetic cardiomyopathy have elevated heart rates and reduced exercise capacity These characteristics can be utilized in screening and diagnosis, he said. In addition, Dr. Poirier also performs ECG, chest radiography and echocardiography, and measures brain natriuretic peptide and microalbuminuria, which are markers of worse prognosis.
For treatment, he aims for strong control of blood pressure, dyslipdemia, and glycemia. Neurohumoral inhibition with ACE inhibitors, beta-blockers, and aldosterone blockers is desirable. He has found that exercise may help normalize diastolic dysfunction, “but the ideal treatment is prevention,” he concluded.
Experiments Explore the Link Between Diabetes and Cardiomyopathy
The causes of diabetic cardiomyopathy are being explored through animal models and, according to Jun Ren, PhD, University of Wyoming, Laramie, Wyoming, United States, oxidative stress may be particularly important. Oxidative stress results from an imbalance between the production and the breakdown of reactive oxygen species. It may occur as a result of hyperglycemia, inflammatory responses, or dyslipidemia. In animal models, Dr. Ren has shown that antioxidants can reverse both morphological and functional abnormalities in diabetic hearts, although antioxidant supplementation in humans has not shown a consistent benefit.
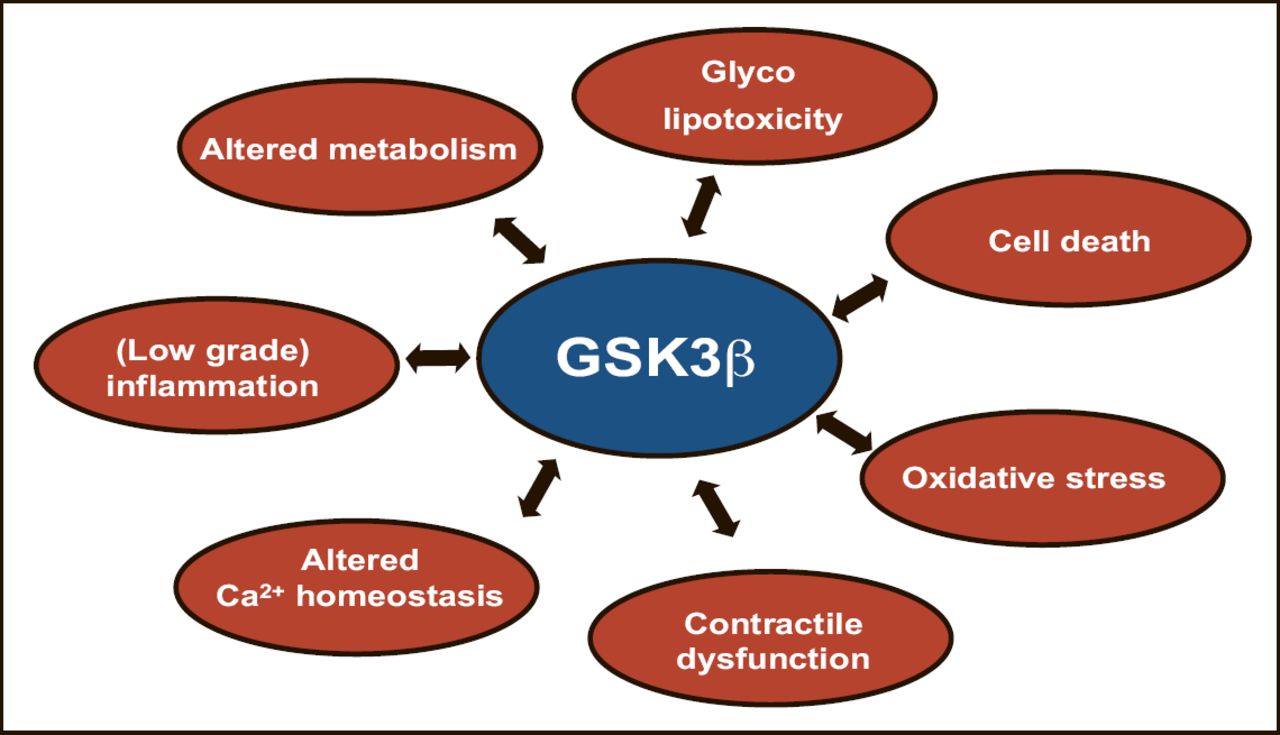
Glycogen synthase kinase 3 (GSK3) may also be important in the pathogenesis of cardiomyopathy. GSK3 is a highly conserved and ubiquitously expressed serine/threonine kinase that has been linked to the regulation of glycogen metabolism and cardiac growth. GSK3β (the most abundant GSK3 in the heart) is overactive in diabetes and insulin-resistant states. Chronic GSK3β overactivity may be detrimental as it may aggravate insulin resistance, induce apoptosis, impair SERA2a/cardiac calcium handling, and interfere with prohypertrophic pathways, said Professor Ronald Vlasboom, VU University Medical Center, Amsterdam, the Netherlands.
The plethora of substrates and signaling cascades impacted by GSK3β renders this kinase a potential therapeutic target (Figure 3). Selective inhibition of GSK3β in animal studies with experimental compounds improved both metabolic and cardiac function, he noted.

Cardiac Hypertrophy: Therapeutic Interventions for antihypertrophic strategies.
Abnormalities in cardiac energy metabolism—in particular, excessive fatty acid metabolism, diminished carbohydrate utilization, and lipotoxicity—may also be part of the pathogenesis, according to Brian Finck, PhD, Washington University School of Medicine, St. Louis, Missouri, United States. His work has focused on a particular nuclear receptor, the peroxisome proliferator-activated receptor (PPARα). PPARα, together with PGC-1α, activates the expression of many genes involved in the uptake, esterification and oxidation of cellular fatty acids and is increased in several mouse models of diabetes.
In a transgenic mouse model of the cardiometabolic phenotype (it has cardiac-specific overexpression of PPARα), Dr. Fink has observed numerous metabolic derangements involving fatty acids and glucose, and an increase in mitochondrial production. These alterations are accompanied by cardiac hypertrophy and ultimately systolic ventricular dysfunction, and they can be exacerbated by a high-fat diet. These findings suggest that abnormalities mediated by PPARα in cardiac energy homeostasis (cardiac fatty acid overload) can be linked to the development of cardiac dysfunction in the diabetic heart.
Trials Explore Clinical Issues of Diabetes-Related Heart Disease
Some oral antidiabetic drugs are believed to be associated with an increased risk of cardiovascular events, but a large retrospective “real world” registry analysis suggests that they may actually possess protective qualities.
Results from the French Registry on Acute ST-Elevation and Non-ST-Elevation Myocardial Infarction (FAST-MI) showed that combined use of metformin plus a sulfonylurea was associated with improved early and 6-month survival after acute myocardial infarction (AMI). The population included 1,316 diabetic patients admitted for an AMI to 223 French intensive care units over a 2-month period. Diabetic patients were categorized according to their use of oral antidiabetic medications prior to admission.
After multivariate adjustments, the best 6-month survival after AMI was found in patients who were admitted while taking both sulfonylureas and metformin. Survival was 95% in this group, compared with 80% in patients who received neither oral agent, for a reduction in risk of 73% (p<0.001). For patients receiving just one agent, survival ranged from 90–95% with the sulfonylurea group faring better than those on metformin alone. Five-day mortality was also significantly improved in the combined treatment group: 0.5% versus 6.1% for users of neither drug (p<0.001), reported Marianne Zeller, MD, Centre Hospitalier Universitaire Dijon, France.
Impact of Hypoglycemia During Hospitalization
Hypoglycemia has been associated with adverse outcomes after AMI, but a study based on the Diabetes Mellitus Insulin-Glucose Infusion in Acute Myocardial Infarction2 (DIGAMI 2) database found no association between treatment-induced hypoglycemia and long-term prognosis.
The DIGAMI 2 population included 1,253 type 2 diabetics from 48 European centers hospitalized for suspected MI. Patients were randomly assigned to treatment with insulin-glucose infusion followed by multi-dose subcutaneous insulin, to insulin-glucose followed by conventional treatment, or to conventional treatment only. After 2 years of follow-up, when researchers adjusted for numerous variables, the occurrence of hypoglycemia during hospitalization (blood glucose <3 mmol/L) had no significant effect on total mortality, cardiovascular mortality, or the composite of death/stroke/reinfarction, reported Linda Melbin, MD, Karolinska Institute, Stockholm, Sweden.
Prof. Melbin maintained that the prospective nature and large size of the cohort support the data's reliability. Her main message was that clinicians should not be afraid to attempt to lower blood glucose during hospitalization.
Adiponectin and Diabetic Complications
Recent studies have reported a relationship between low adiponectin levels and cardiovascular disease. However, an international study showed that low adiponectin levels do not provide additional predictive value beyond established cardiovascular risk factors.
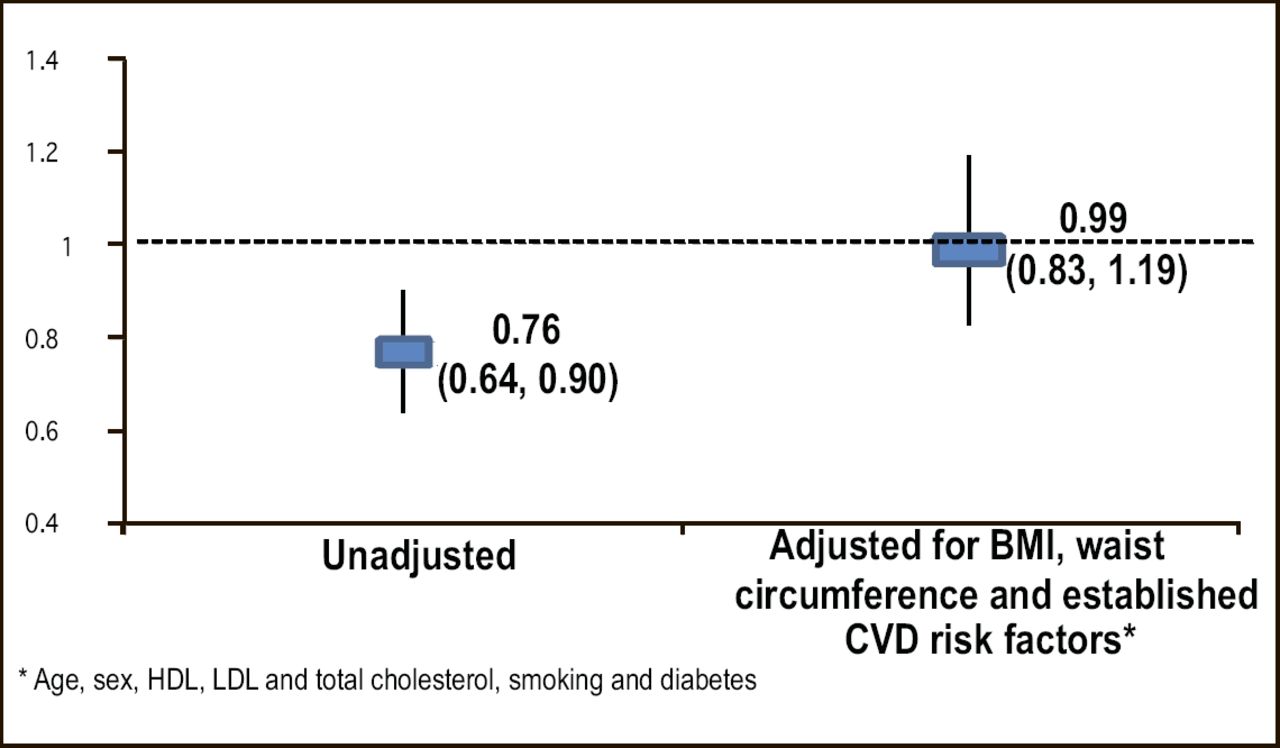
Investigators from the Quebec Heart Institute reported the results of a prospective case-control analysis nested in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk cohort. The study population included 1,034 adults who were healthy at baseline but developed coronary artery disease over time matched with 1,919 controls who remained disease-free. Baseline non-fasting plasma adiponectin concentrations were found to be significantly lower in cases than in matched controls (p=0.005) and to increase the risk for future events (p<0.001). However, after adjustment for body mass index, waist circumference and established cardiovascular disease risk factors, these relationships were no longer significant (Figure 5).

Odds Ratio for Future Coronary Artery Disease (Men and Women).
The risk of developing coronary artery disease was more closely related to the presence of a high waist circumference and low HDL levels than to low adiponectin levels, reported Mélanie Côté, MD, Hospital Laval, Quebec, Canada.
Improving Risk Calculations Through Genotyping
Traditional calculations of cardiovascular risk, such as the Framingham Risk Score, only accurately predict events only in a minority of subjects. Investigators from the United Kingdom evaluated whether a set of common variants in genes previously found related to coronary heart disease risk might enhance the utility of such algorithms. In a multivariate analysis, they found that several genes significantly (p<0.001) improved the predictive utility of such algorithms, including those related to uncoupling protein 2, apolipoprotein E, lipoprotein lipase, and apolipoprotein A4, as well as several genes showing interaction with smoking, interleukin-6 and platelet/endothelial cell adhesion molecule genotypes. In the future, risk estimates may include not only conventional risk factors but also a panel of selected genotypes concluded Philippa Talmud, PhD, University College London, United Kingdom.
Severe Mental Illness and Type 2 Diabetes
The prevalence of diabetes among patients with severe mental illness is 2–3 times higher than that for the general population. While this disproportionate risk has largely been attributed to treatment with atypical antipsychotic agents, Stephen Gough, MD, University of Birmingham, UK, said, “I think the link goes well beyond this.”
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
- Article
- Summary
- Diabetic Cardiomyopathy
- Experiments Explore the Link Between Diabetes and Cardiomyopathy
- Trials Explore Clinical Issues of Diabetes-Related Heart Disease
- Impact of Hypoglycemia During Hospitalization
- Adiponectin and Diabetic Complications
- Improving Risk Calculations Through Genotyping
- Severe Mental Illness and Type 2 Diabetes
- Figures & Data
- Info & Metrics
- eLetters
Cited By...
- No citing articles found.