

Summary
The metabolic syndrome represents a cluster of risk factors (ie, obesity, hypertension, elevated triglycerides, low high-density lipoprotein-cholesterol, and insulin resistance) which lead to an increased risk of heart disease, stroke, and type 2 diabetes. The effects of lifestyle and pharmacologic interventions were discussed during this special session held in collaboration with the World Metabolic Syndrome Project.
- cardiometabolic disorder
The metabolic syndrome represents a cluster of risk factors (ie, obesity, hypertension, elevated triglycerides, low HDL-cholesterol, and insulin resistance) which lead to an increased risk of heart disease, stroke, and type 2 diabetes. The effects of lifestyle and pharmacologic interventions were discussed during this special session held in collaboration with the World Metabolic Syndrome Project.
According to Jean-Pierre Després, PhD, Quebec Heart Institute, Canada, intra-abdominal or visceral fat, more than overall weight, plays a significant role in the development of the metabolic syndrome [Després J-P and Lemieux I. Nature 2006]. He reported on the results of a program developed to assess the effect of lifestyle modification in the clinical management of viscerally obese men. Patients (n=185) saw a dietician and an exercise physiologist once per month. After 1 year, there was a significant reduction vs baseline in both subcutaneous (19%) and visceral fat (29%) (both p<0.0001) accompanied by an overall reduction of 7 kg in body weight and an 8.6 cm decrease in waist circumference. Significant improvements were also seen in all of the risk factors associated with the metabolic syndrome (Table 1).
Changes in Risk Factor Levels After 1 Year of Diet and Exercise.
Particularly important was the finding that changes in visceral fat could not be predicted by changes in body weight.
According to Dr. Després, “We need to go beyond body weight, beyond healthy weight, beyond BMI. We need to increase energy expenditure, which will in turn reduce visceral adipose tissue and lower the risk for cardiovascular disease and diabetes.”
Philip Barter, MD, The Heart Research Institute, Sydney, Australia, discussed pharmacologic interventions in the management of the risk factors associated with the metabolic syndrome.
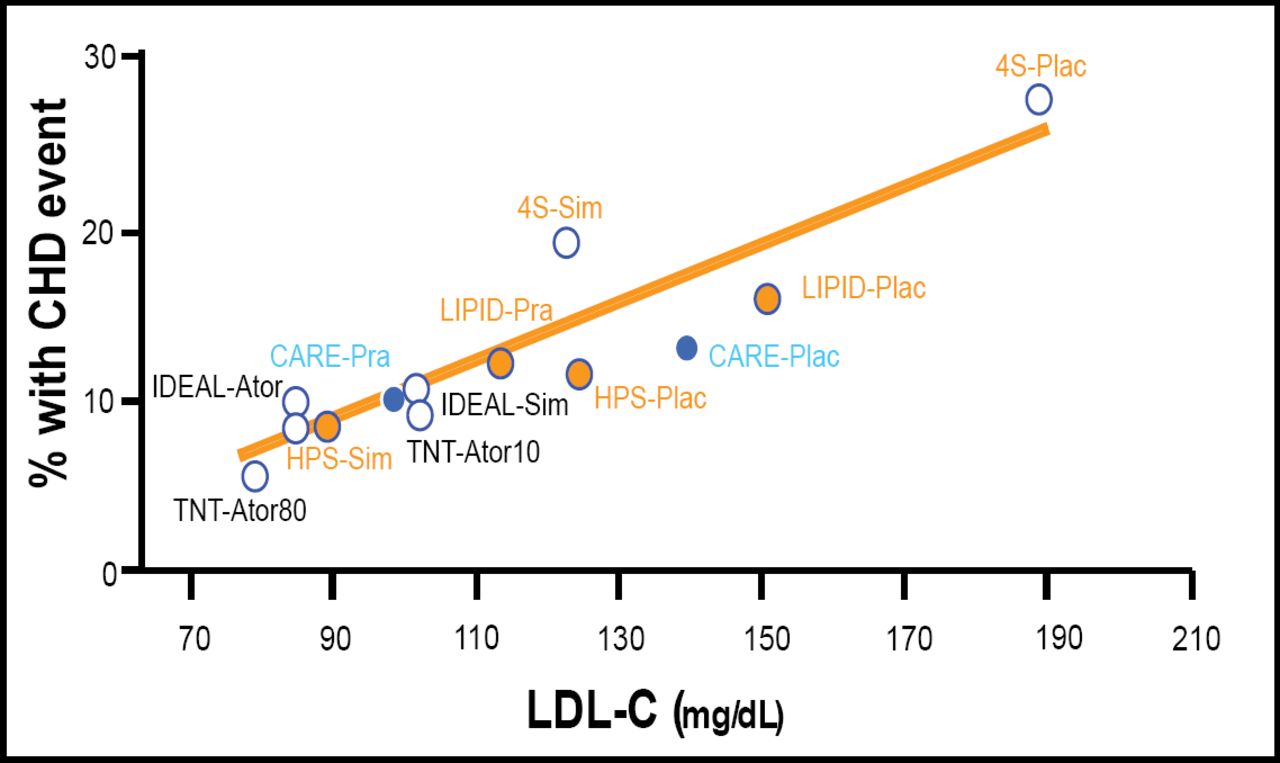
Numerous studies have proven that statins reduce cardiovascular events (Figure 1).

Statin Trials: LDL-C Levels vs Events.
Deedwania and colleagues have shown, however, that intensive lowering of LDL-C produced even greater benefit in patients with both coronary heart disease and the metabolic syndrome. Their analysis comprised data from 5,584 patients randomly assigned to receive either atorvastatin 10 mg (n=2,820) or 80 mg per day (n=2,764). Although at a median follow-up of 4.9 years, irrespective of treatment assignment, significantly more patients with metabolic syndrome (11.3%) had a major cardiovascular event than those without metabolic syndrome (8.0%; p<0·0001); the increased risk was significantly reduced by intensive therapy, as shown by significantly fewer events in patients receiving atorvastatin 80 mg (262, 9.5%) vs those receiving the lower dose (367, 13%) (HR 0·71; 95% CI 0·61, 0·84; p<0·0001) [Deedwania P et al. Lancet 2006].
Several studies that assessed the efficacy of fibrates in the treatment of patients with the metabolic syndrome such as the Helsinki Heart Study [Tenkanen L et al. Circulation 1995; Manninen V et al. Circulation 1992], the VA-HIT Study [Rubins HB et al. Arch Int Med 2002], and the BIP study [BIP Study Group. Circulation 2000], have shown that the benefits of fibrates were greatest in people with risk factors for the metabolic syndrome such as increased body weight, particularly if associated with low LDL-C, elevated plasma triglycerides, and elevated fasting plasma insulin levels.
According to Dr. Barter, although, theoretically there may be advantages to using statins and fibrates in combination, and studies are underway, this has not been proven. Furthermore, combination of high-dose statins and fibrate (in particular gemfibrozil) has been shown to increase the risk of rhabdomyolysis. Other pharmacologic approaches such as the cannabinoid-1 receptor blockers (rimonabant) are also being investigated but their efficacy in reducing cardiovascular events has not yet been demonstrated.
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.