

Summary
The gold standard for the diagnosis of coronary artery disease (CAD) has been conventional coronary angiography. However, multislice computed tomography (MSCT) has shown promise as a less invasive diagnostic modality. This article presents the results of a prospective management outcome study to evaluate the safety of ruling out CAD on the basis of normal findings on MSCT
- cardiac imaging techniques
- tomography
- radiography
- coronary artery disease
- imaging modalities

The gold standard for the diagnosis of coronary artery disease (CAD) has been conventional coronary angiography. However, multislice computed tomography (MSCT) has shown promise as a less invasive diagnostic modality. When compared with conventional angiography in patients with suspected CAD, MSCT (4-,16-, and 64-slice) has been associated with a sensitivity of 85–99%, a specificity of 95–97%, a positive predictive value of 76–97%, and a negative predictive value of 97% [Schuijf JD et al. Am Heart J 2006]. In addition, the use of MSCT avoids the complications, discomfort, and expense associated with conventional angiography; 64-slice CT has the additional advantage of quick (13 second) imaging that reduces motion artifact and thus further improves accuracy. As such, MSCT has the potential to play an important role in ruling out CAD in a less invasive and more cost-effective manner.
Martine Gilard, MD, Brest University Hospital, Brest Cedex, France, presented the results of a prospective management outcome study to evaluate the safety of ruling out CAD on the basis of normal findings on MSCT. In this study, 200 patients scheduled for conventional coronary angiography were evaluated with MSCT; 141 patients with normal findings on MSCT were followed up for a mean of 14.7 months (range, 6–26 months). The outcomes for these patients were compared with those for patients with normal findings on coronary angiography.
Prof. Gilard reported that there were no deaths, one myocardial infarction (0.7%), and five referrals for conventional angiography (3.5%). These results compare favorably with those reported in the literature with normal conventional angiography [Lichtlen PR et al. J Am Coll Cardiol 1995].
Among the five subsequent angiographies, two demonstrated normal results and three showed evidence of significant lesions. Thus, 137 (97.2%) of the 141 patients was clinically event-free, leading Prof. Gilard and colleagues to conclude that for individuals with suspected significant CAD, MSCT can be used alone to safely rule out this diagnosis.
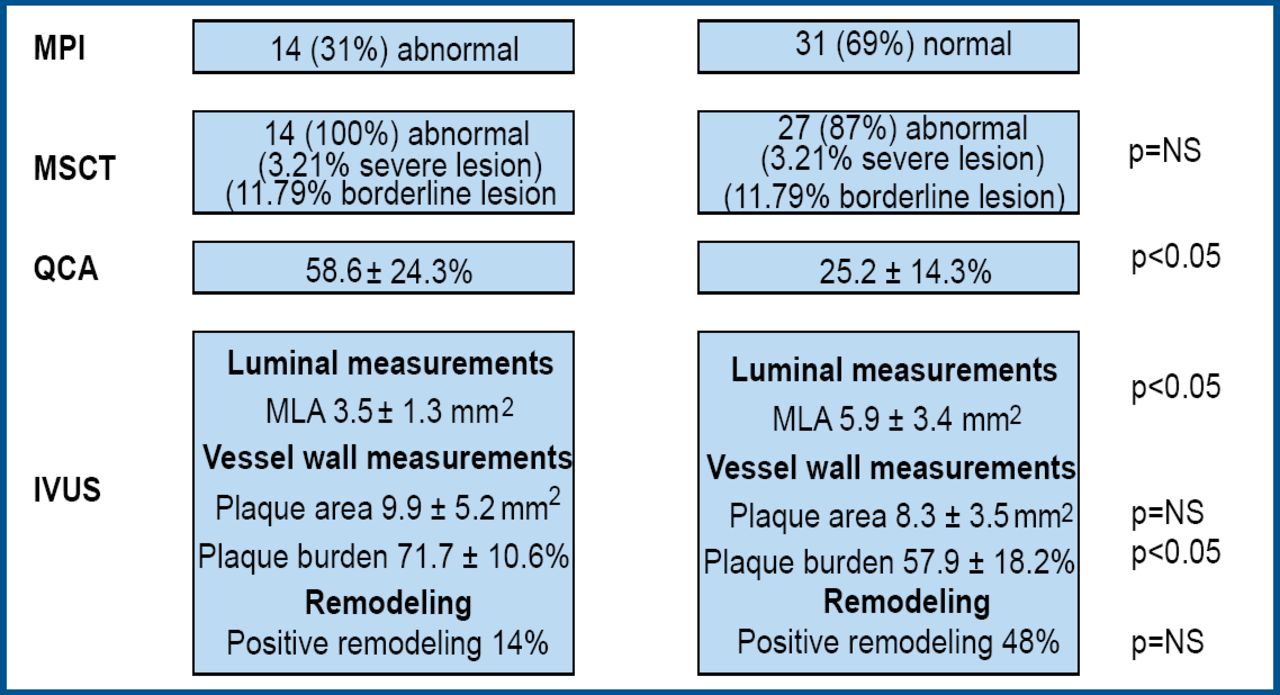
In another presentation, Joanne D. Schuijf, MD, Leiden University Medical Center, the Netherlands, reported on a study in which the severity of CAD as determined by MSCT, quantitative coronary angiography (QCA), and intravascular ultrasound (IVUS), was evaluated in relation to functional assessment with myocardial perfusion imaging (MPI). Prof. Schuijf remarked that MSCT provides evidence of atherosclerosis whereas MPI is designed to detect ischemia, which explains why patients with abnormal findings on MSCT frequently have normal MPI.
Prof. Schuijf reported that there was good agreement among the modalities for patients with advanced CAD (exhibiting ischemia on MPI) but that the findings were frequently discrepant for patients with mild atherosclerosis (Figure 1).

MPI vs MSCT vs QCA vs IVUS.
For example, some patients had no ischemia according to MPI and no significant stenosis on QCA but had evidence of atherosclerosis on MSCT and intravascular ultrasound. Prof. Schuijf concluded that the complementary nature of MPI and MSCT may allow for improved characterization of CAD. She added that more evidence is needed before it can be determined whether the combined use of the two modalities will result in improved management and outcome.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.