

Summary
For patients with ST-elevation myocdardial infarction (STEMI), reperfusion with primary PCI is recommended if it can be performed within 90 minutes. However, treatment within this narrow window can not always be achieved, especially for patients who present to a hospital without a PCI facility. Fibrinolytic therapy is still the preferred treatment in this setting. The Combined Abciximab Reteplase Stent Study in Acute Myocardial Infarction [CARESS] trial was designed to compare a strategy of early transfer after fibrinolysis versus a strategy of medical treatment and transfer for PCI only if there was no evidence of reperfusion.
- myocardial infarction clinical trials
- interventional radiology
- thrombotic disorders
- interventional techniques & devices
For patients with ST-elevation myocdardial infarction (STEMI), reperfusion with primary PCI is recommended if it can be performed within 90 minutes. However, treatment within this narrow window can not always be achieved, especially for patients who present to a hospital without a PCI facility. Fibrinolytic therapy is still the preferred treatment in this setting. The CARESS (Combined Abciximab Reteplase Stent Study in Acute Myocardial Infarction) in AMI trial was designed to compare a strategy of early transfer after fibrinolysis versus a strategy of medical treatment and transfer for PCI only if there was no evidence of reperfusion.
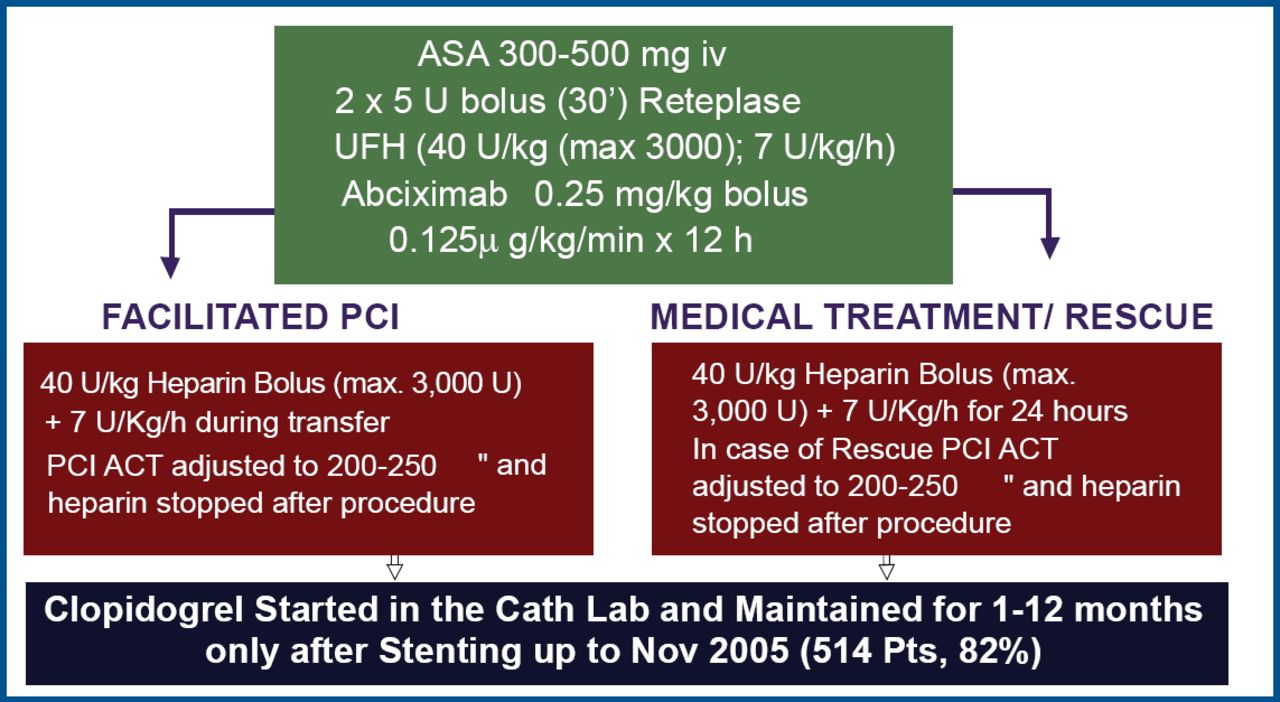
Carlo Di Mario, MD, Imperial College, London, UK, reported the findings of the CARESS in AMI study, which was carried out in hospitals in Italy, Poland, and France that did not have PCI facilities. Six hundred patients with STEMI who presented less than 12 hours after symptom onset were randomly assigned to either facilitated PCI or medical treatment/rescue after fibrinolysis with half-dose reteplase and abciximab (Figure 1). The primary outcome was the composite of all-cause mortality, reinfarction, or refractory ischemia at 30 days. Of the patients in the medical treatment/rescue group, 36% were subsequently referred for PCI.

CARESS Treatment Summary.
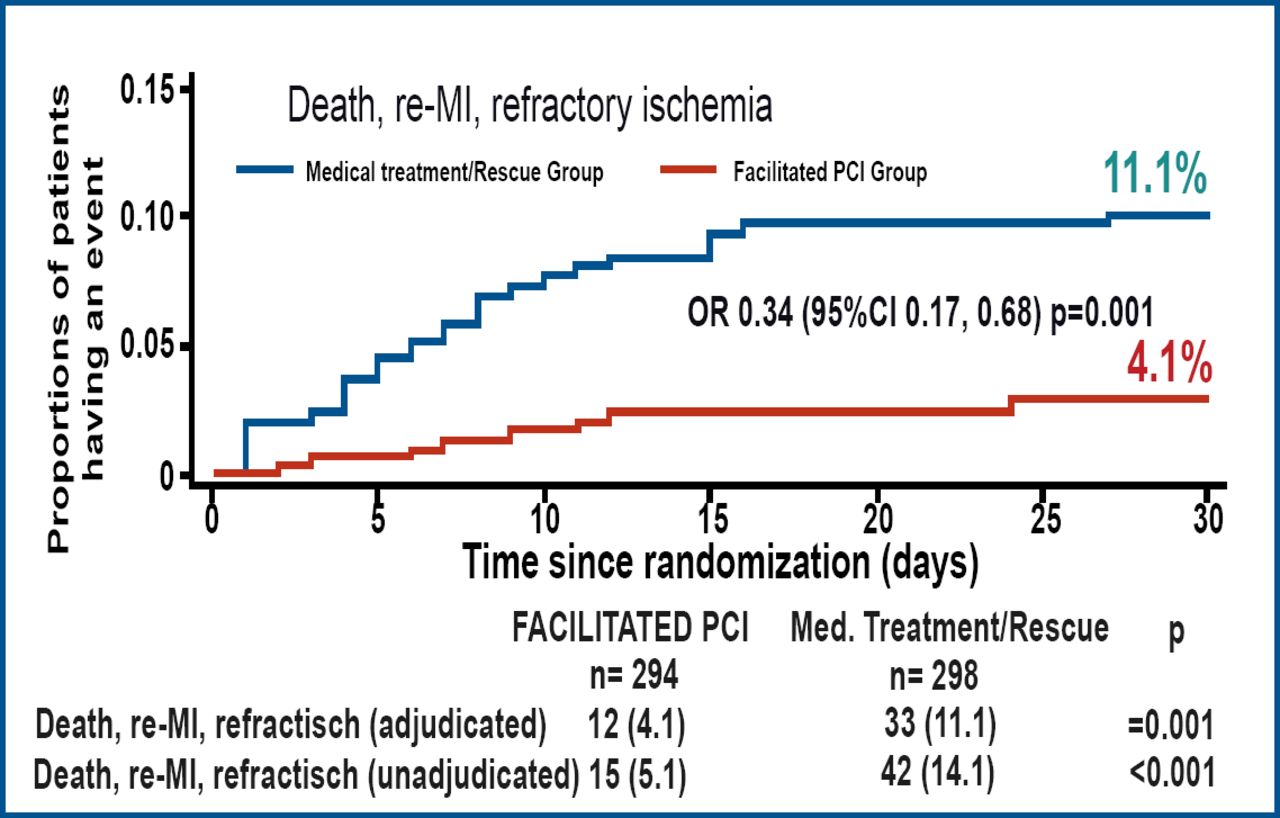
Prof. Di Mario reported that facilitated PCI (with half-dose reteplase + abciximab) led to a 67% reduction in the incidence of the composite endpoint (Figure 2) compared to medical treatment with half-dose reteplase + abciximab followed by rescue PCI as needed. When the components of the primary endpoint were assessed individually, refractory ischemia was significantly less frequent in the facilitated PCI group (0.7% vs 5.0%; p<0.002). The incidences of death and reinfarction were also lower in the facilitated PCI group, but these differences did not reach statistical significance (3.1% vs 4.4%, p=0.403, and 0.3% vs 1.7%, p=0.104, respectively). Severe bleeding was rare in both groups, and Prof. Di Mario suggested that this was because the study excluded older patients and patients at high risk for bleeding.

Primary Outcome at 30 Days.
“In our view,” concluded Prof. Di Mario, “this trial confirms and expands the indication of the current ESC guidelines to perform early angioplasty, within 24 hours after lysis, and suggests that high-risk STEMI patients should be immediately transferred for angiography after lysis.”
Professor Freek Verheugt, Nijmegen University, the Netherlands, who discussed the study, noted that the results of CARESS confirmed the findings of other studies that have indicated the benefit of immediate PCI. He said that one of the remaining questions is how the results would have differed if all patients had been given clopidogrel. In addition, he noted that an important factor to determine is the optimal time interval between fibrinolysis and PCI. This interval has ranged from 2.3–17 hours in trials showing benefit of facilitated PCI.
One of the limitations of the CARESS trial was the absence of a standard strategy (eg, full-dose fibrinolytic or primary PCI without preceding fibrinolysis) as the comparator. Without such an “anchor” to serve as the gold-standard, it is possible that neither of the strategies tested in CARESS would be superior to currently recommended reperfusion strategies. Such a scenario would be consistent with the findings of the GUSTO-V (half-dose rPA + abciximab was not superior to full-dose rPA) and FINESSE (half-dose rPA + abciximab prior to PCI was less beneficial than primary PCI with abciximab in the catheterization laboratory) studies, thus emphasizing the importance of including existing standard treatments in trials that are evaluating novel therapies.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.