

Summary
It is well known that patients with rheumatoid arthritis (RA) have an increased risk of fatal and non-fatal acute myocardial infarction (AMI). Endothelial dysfunction is part of the RA disease process and is mediated by TNF-alpha [Hurlimann D et al. Circulation 2002]. Localized inflammatory responses in the intimal layer of the arterial wall have been shown to be responsible for many aspects of intimal thickening and plaque disruption, leading to acute cardiovascular events. TNF inhibitors may reduce the risk of AMI in RA patients because their strong anti-inflammatory effect improves endothelial function [Bacon PA et al. Int Rev Immunol 2002].
It is well known that patients with rheumatoid arthritis (RA) have an increased risk of fatal and non-fatal acute myocardial infarction (AMI). Endothelial dysfunction is part of the RA disease process and is mediated by TNF-alpha [Hurlimann D et al. Circulation 2002]. Localized inflammatory responses in the intimal layer of the arterial wall have been shown to be responsible for many aspects of intimal thickening and plaque disruption, leading to acute cardiovascular events. TNF inhibitors may reduce the risk of AMI in RA patients because their strong anti-inflammatory effect improves endothelial function [Bacon PA et al. Int Rev Immunol 2002].
The risk of AMI with TNF-inhibitor therapy, methotrexate (MTX), and other DMARDs was studied by Gurkirpal Singh, MD, Standford University School of Medicine, in a large population (MediCal, the Medicaid program for California) of patients with RA, many of whom were on concomitant aspirin therapy.
Cases of acute myocardial infarction (AMI) were risk-set matched with 4 controls for age, gender, and date of AMI. All analyses were adjusted for 38 confounding risk factors (including surrogate variables for smoking and dyslipidemias) as well as concomitant aspirin and NSAID treatment (prescription or over-the-counter use).
A total of 19,233 RA patients (mean age 54.7 years, 79.4% women) were identified. Of these, 13,383 patients took MTX, 14,958 took other DMARDs, and 4,943 took TNF inhibitors. Treatment groups included TNF inhibitors (monotherapy), TNF inhibitors plus MTX, TNF inhibitors plus non-MTX DMARDS, non-MTX DMARDs alone, and MTX plus non-TNF DMARDs.
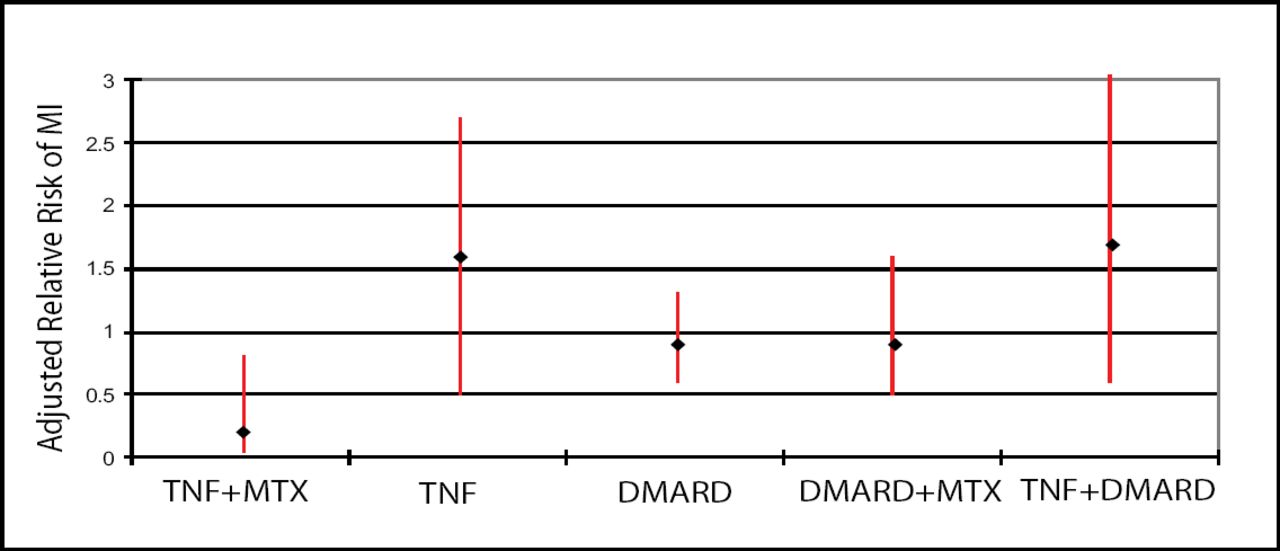
During 74,006 person-years of follow-up, 441 cases of AMI were identified, of which 8% were fatal. Treatment with TNF inhibitors plus MTX significantly reduced the risk of AMI vs MTX monotherapy (multivariate-adjusted relative risk 0.20 (95% CI 0.05 − 0.88, p<0.03; Figure 1). No statistical difference was seen with TNF-inhibitor monotherapy (RR 1.17, 95% CI 0.50–2.75), TNF-inhibitor with other DMARDs (RR 1.78, 95% CI 0.60–5.27), other DMARD therapies without MTX (RR 0.88, 95% CI 0.60–1.31) or a combination of DMARDs and MTX (RR 0.93, 95% CI 0.54–1.62) vs MTX monotherapy. Systemic corticosteroid use was an independent risk factor which significantly increased the risk of AMI (adjusted RR 1.37, 95% CI 1.07–1.75, p<0.01).
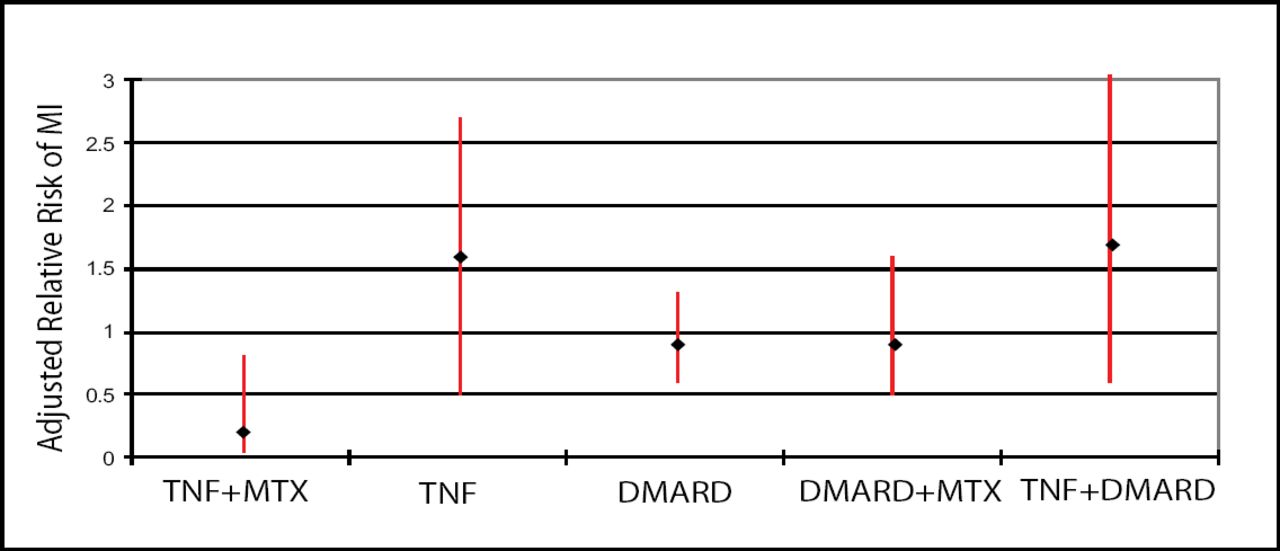
Adjusted Relative Risk of AMI, Compared to MTX Monotherapy.
These results indicate that combination therapy using a TNF-inhibitor plus MTX is associated with a reduction in the risk of acute myocardial infarction by 80% vs MTX monotherapy in patients with RA. Such a dramatic effect enhances the therapeutic gains of TNF-inhibitor therapy in patients with RA and should be seriously considered, particularly in high-risk patients.
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.