

Summary
Cancer is a global health problem. The majority of cancer-related studies focus on diagnosis and treatment, but only a minority of the world's population benefit from these strategies. Primary prevention is, therefore, essential to cancer control. In more developed countries, cancer rates are dropping, but in developing countries, the reverse is true. This trend is due not only to scarce resources, but also to a general lack of prevention knowledge.
- Breast Cancer
- Reproductive Cancers
- Vaccinations
- Gastrointestinal Cancers
- Cancer
- Affordability of Care
- Smoking Cessation
- Respiratory Cancers
Cancer is a global health problem. The majority of cancer-related studies focus on diagnosis and treatment, but only a minority of the world's population benefit from these strategies. Primary prevention is, therefore, essential to cancer control. In more developed countries, cancer rates are dropping, but in developing countries, the reverse is true. This trend is due not only to scarce resources, but also to a general lack of prevention knowledge.
Lung Cancer Prevention
Smoking is not only the main cause of cancer in the world, it is also the main cause of death in adult life worldwide.
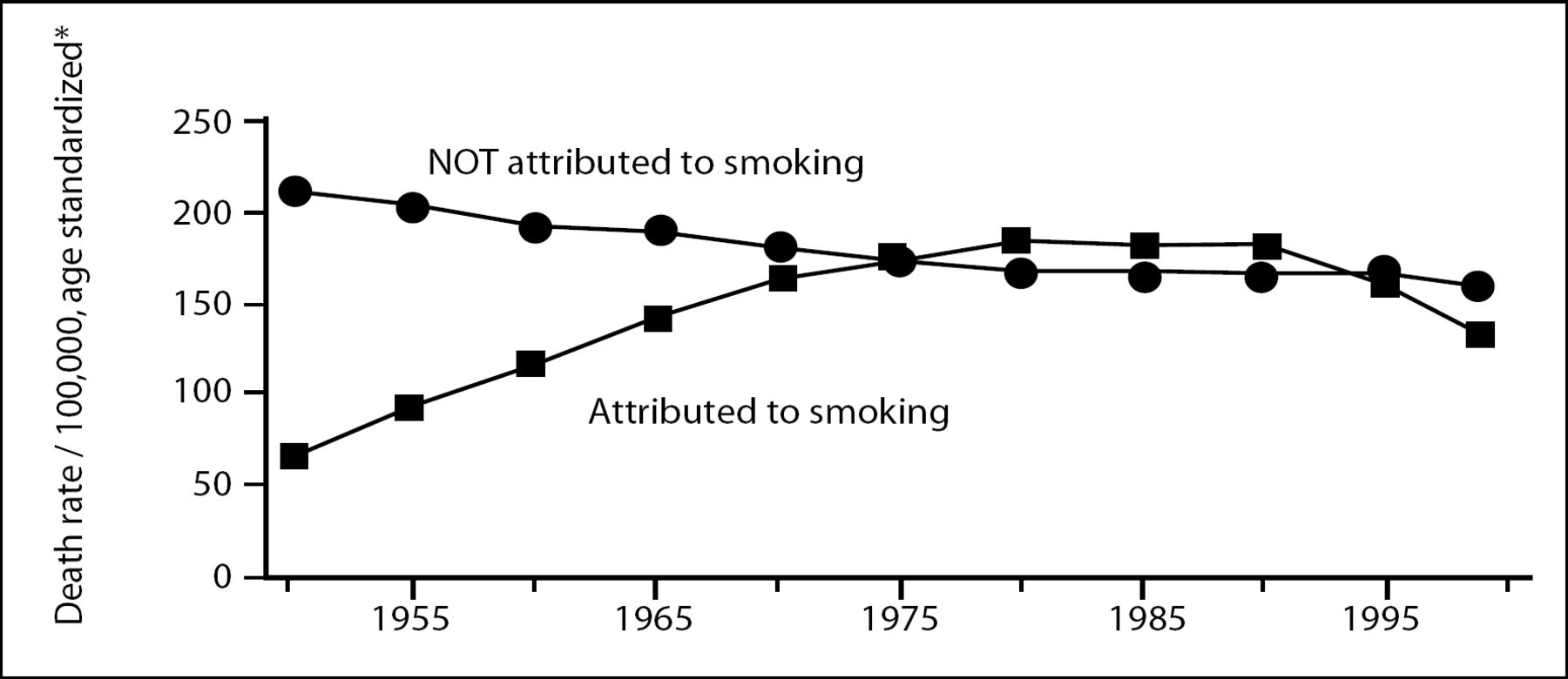
“Stopping smoking works,” emphasized Richard Peto, FRS, University of Oxford, citing a provocative study conducted by Doll et al [Doll R et al. BMJ 2004]. The key to cancer prevention in the next few decades, he urges, is through smoking cessation; smoking prevention in children will lead to a drop in cancer rates in the second half of this century. Indeed, US mortality data from the Centers for Disease Control (Figure 1) show that from 1950–1980, mortality from lung cancer increased steadily, correlating with an increase of smokers. From 1980–1999, however, when emphasis was placed on smoking cessation, mortality rates decreased dramatically.
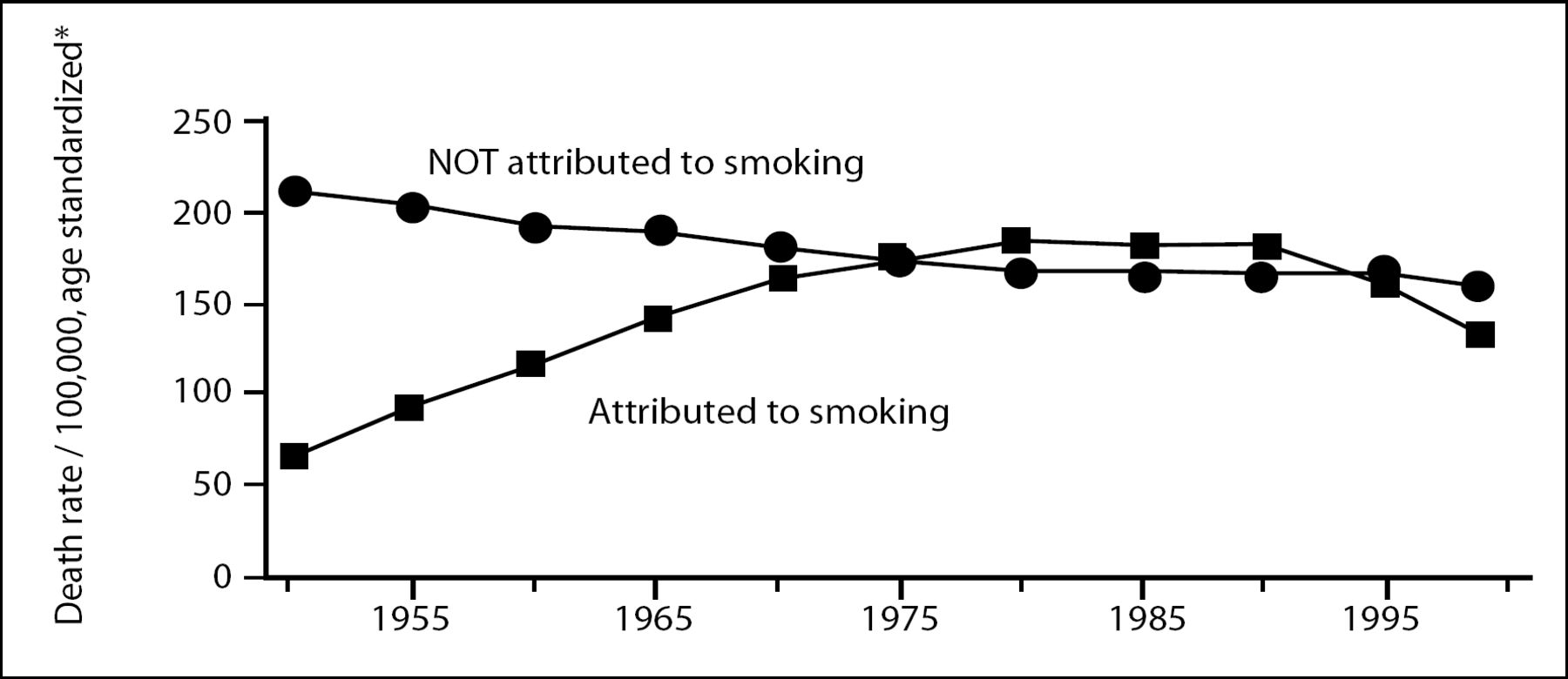
US 1950–1999 Mortality Data from Lung Cancer.
There are about thirty million new smokers worldwide each year in the US, half of which will be killed if they continue. At that rate, 10 million deaths would occur each year, or 100 million per decade. Therefore, prevention of the estimated 450 million tobacco deaths before the year 2050 requires adult cessation; this necessitates serious implementation of tobacco control throughout the world, particularly in developing countries where such strategies have been inadequate.
Breast Cancer Prevention
Fifty-percent of the world's 6.5 billion people are women; 79% of these women are less than 50 years old, and 52% are less than 30 years old. However, the preventative agents that are currently being evaluated are being investigated in high-risk women over 50. Therefore, the current targeted population of women in which to prevent breast cancer is only 21% of the world's 3.28 million women.
“I consider it highly appropriate that preventative agents be considered for use in younger women,” concludes Bernard Fisher, MD, University of Pittsburgh School of Medicine, adding that there are 411,000 deaths due to breast cancer worldwide per year.
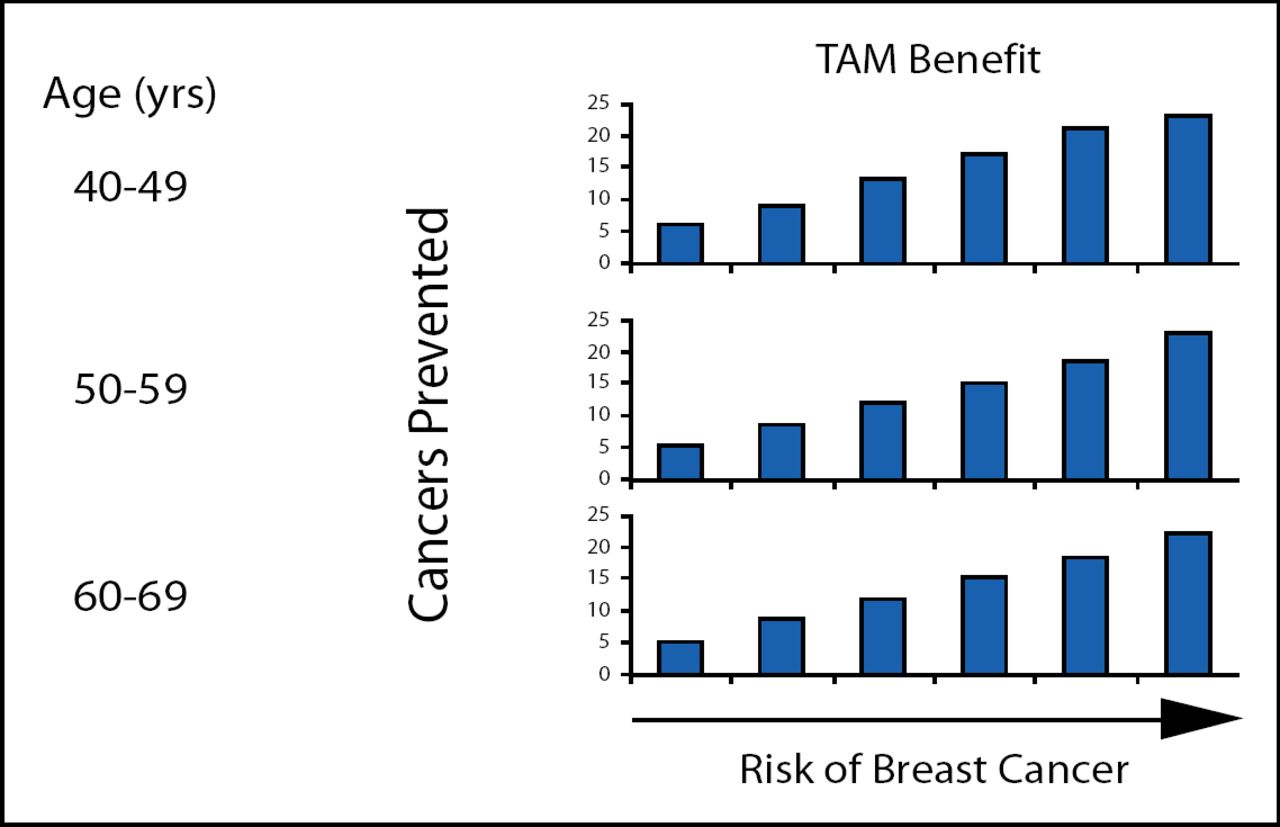
Five randomized trials have been conducted to look at the prevention of breast cancer: NSABP-1 + NSABP-2, IBIS-1, Royal Marsden and an Italian study. The NSABP-1 trial compared placebo to tamoxifen (TAM) in women at increased risk. The investigators of this study observed no difference at onset, but superiority of the TAM arm after 2 years and through 7 years. This study provided the first evidence that breast cancer can be prevented in women at increased risk for the disease and this benefit increased over time. Most striking was the 69% reduction in the occurrence of ER+ tumors. Additionally, this study provided the first algorithm for indicating breast cancer risk and showed that the higher the risk of breast cancer, the more a patient benefited from TAM treatment (Figure 2).
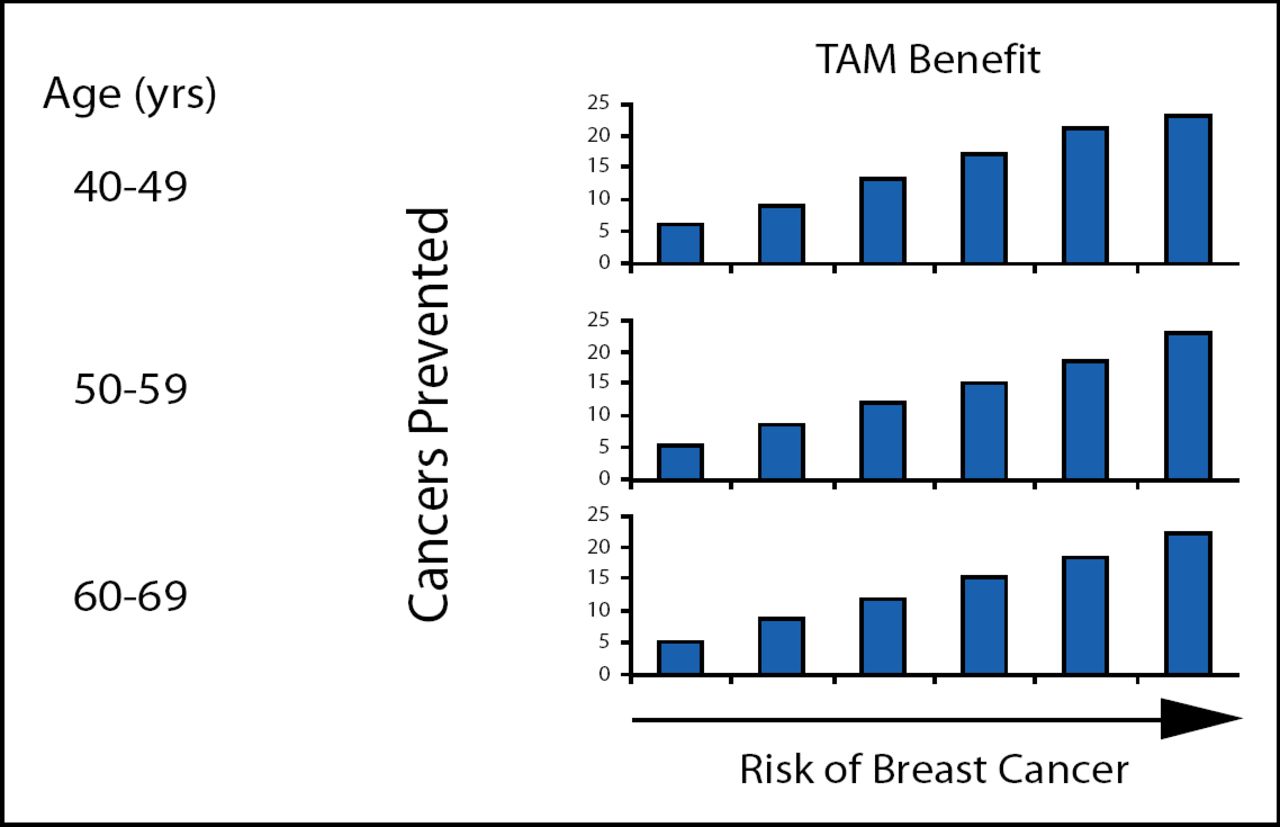
TAM Benefit in Breast Cancer.
“Only once before in my 50 years of experience in breast cancer prevention trials have I observed such compelling findings…” remarked Dr. Fisher.
Results from the NSABP-2 with raloxifene showed similar results to those of TAM. Additionally, IBIS-1, the Royal Marsden study and an Italian study all confirmed the results of NSABP-1 comparing TAM to placebo in the prevention of breast cancer in high risk patients.
Colon Cancer Prevention
There are several risk factors in colon cancer that cannot be controlled, including age, family history, inflammatory bowel disease, and history of adenomatous polyps. However, there are many risk factors that can be controlled with screening and the adoption of a healthy lifestyle. First, polypectomy has been shown to reduce the incidence of colon cancer by 75–90% [Winawer SJ et al. New Eng J Med 1993]. However, due to the unpleasant nature of colonoscopies, a noninvasive stool DNA test is being developed. Non-steroidal anti-inflammatory drugs have also reduced the incidence of colorectal polyps, colon cancer and colon cancer mortality.
Nutrition and diet undoubtedly contribute to colon cancer risk. Increases in serving size and soda consumption have contributed to obesity worldwide over the past few decades; this trend needs to be reversed. Additionally, some studies suggest that fiber, vitamin D [Gorham et al. J Steroid Biochem Mol Biol 2005], calcium [Baron et al. N Eng J Med 1999] and folate [Giovannucci et al. Ann Intern Med 1998] reduce the relative risk of colon cancer.
Cervical and Hepatic Cancer Vaccines
Vaccination is one of the most effective ways of preventing disease. “A vaccine to prevent cancer is an oncologists dream”, comments Hakan Mellstedt, MD, Karolinska Hospital, Sweden, though it works in only very specific cases. When a virus is an essential part of tumor development, such as in the cases of cervical and hepatic cancers, this strategy can be very successful.
Approximately 190,000 women die from cervical cancer each year; 78% of these deaths occur in developing countries. Human papilloma virus (HPV) is considered to be necessary for the development of cervical cancer, specifically subtypes 16 and 18. A study by Koutsky et al [Koutsky et al. N Engl J Med 2002] was the first to show 100% efficacy of a monovalent HPV vaccine against strain 16 infections; follow-up studies confirmed these results. Two vaccines have thus been commercially developed: Gardasil by Merck & Co/Sanofi-Aventis, and Cervarix by GlaxoSmithKline. Table 1 shows the combined efficacy results of Gardasil in four major trials.
Summary of Efficacy Studies of Gardasil in the per Protocol Populations (005, 007, 013, 015).
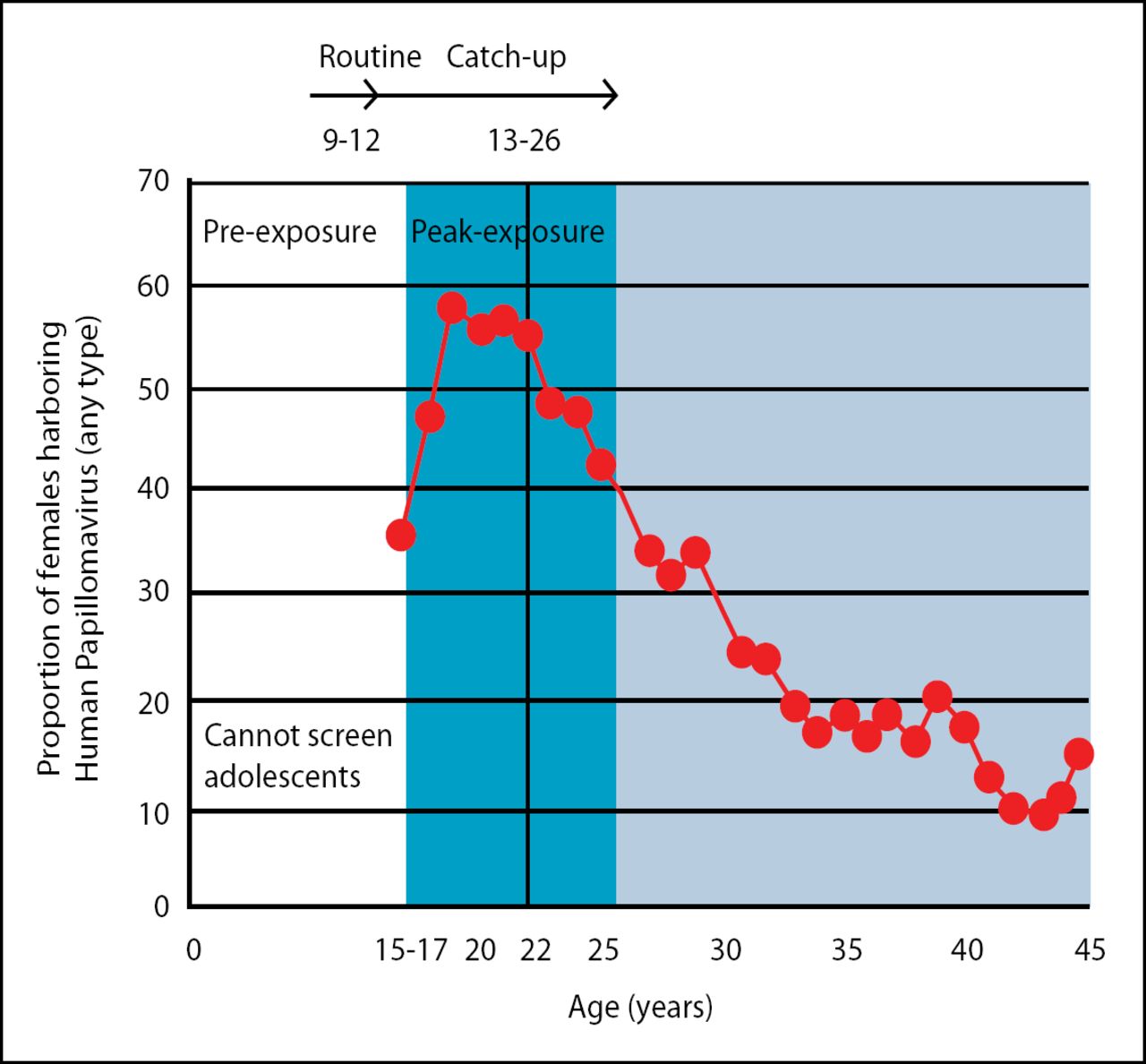
The appropriate age at which to vaccinate has been controversial. Studies have shown that the ideal age range is between 9 and 12 years old (Figure 3), though some people feel this is too young for a vaccine of this nature. It is possible to some extent to play catch up for ages 13–26, but either way the vaccine must be given prior to exposure. It should be noted, however, that the vaccine is not a substitute for routine Pap smear screening.
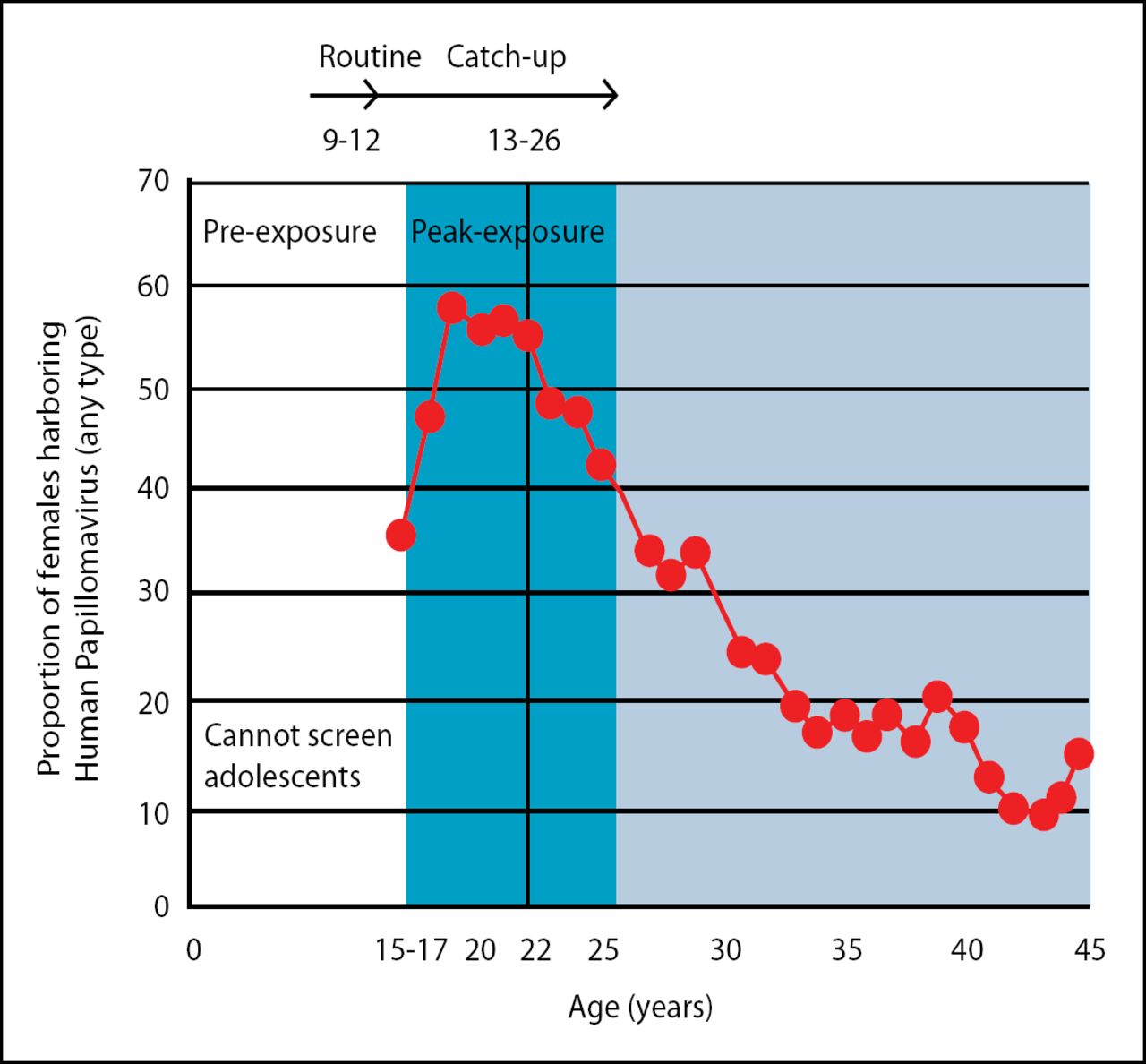
HPV Vaccine Efficacy By Age.
Another virus that causes cancer is the hepatitis B virus (HBV); this virus causes liver cancer. Approximately two billion people are currently infected with HBV and there are 500,000–700,000 HBV-related deaths each year.
A vaccination for HBV was introduced in 1984 in Taiwan, and by 1986 it was administered to all newborns. The vaccine had tremendous success; the incidence of hepatocellular carcinoma decreased from 9.8% in 1984 to 0.7% in 1999. Future goals are to introduce the HBV vaccine in all countries with adequate delivery systems by the end of 2007, and to have coverage of 90% by 2010.
In conclusion, HPV- and HBV-related carcinomas are preventable with vaccines. For full efficacy, vaccination must be initiated prior to infection, though the duration of protective immunity has not been established and boost immunizations are likely to be necessary.
A Global Action: The UICC role
In May of 2005, a general assembly of WHO-member states accepted an unprecedented resolution, “Cancer prevention and control” which prioritizes cancer control. Additionally, the International Union against Cancer (UICC) has outlined four goals related to cancer prevention:
1) to give children a smoke free world
2) to encourage a healthy diet and physical
3) to educate communities on vaccines that prevent cancer-causing viruses
4) to promote “sun smarts” by avoiding UV exposure
Since today's children are tomorrow's world, cancer prevention should undoubtedly be a priority.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.