

Summary
Which is better: psychotherapy, pharmacotherapy, or a combination of the two? This article presents two differing views on this subject from a psychodynamic clinician's perspective. The psychodynamic model is derived from psychoanalysis, an intensive therapy that seeks to explore the unconscious to reveal to the patient the source of their psychiatric symptoms.
- Psychopharmacology
Which is better: psychotherapy, pharmacotherapy, or a combination of the two? Two experts gave a candid and entertaining presentation of their views on the subject at a session devoted to this topic. Steven P. Roose, MD, Columbia University, gave the psychodynamic clinician's perspective. The psychodynamic model is derived from psychoanalysis, an intensive therapy that seeks to explore the unconscious to reveal to the patient the source of their psychiatric symptoms. “When medication was first introduced it was (not surprisingly) greeted in the [psycho] dynamic community with outright hostility, often suspicion. Medication was considered to be only for symptomatic relief, putting a bandage on the problem,” noted Dr. Roose. The perception was that if you relieved that patient's symptoms of anxiety or depression that all motivation would be taken away. Over time this has changed. Dr. Roose presented data from the most recent 67 patients who came to the psychodynamic clinic at Columbia:
Current Diagnoses: 54% with anxiety disorders, 36% with major depressive disorder, 12% with dysthymia.
Comorbid diagnoses: 31% with mood and anxiety disorders, 23% with anxiety disorders, 22% with mood disorders.
Lifetime Diagnoses: 81% with mood disorders and 54% with anxiety disorders
In Dr. Roose's opinion, these findings suggest that psychoanalysis or psychodynamic therapy is being sought out by patients with mood and anxiety disorders who have not obtained relief using other methods. Surveys at Columbia and other institutions indicate that psychodynamic therapists now prescribe medication for the patients who need it, and that both the disorder and the psychoanalytic process improve as a result of the pharmacotherapy. “You can't do dynamic treatment or psychoanalysis in patients who are significantly depressed. In other data there was a very powerful, significant inverse correlation between the scales that measure what is referred to as psychological mindedness, the capacity for insight, and the ability to think psychologically about oneself, and one's depression scores. “The more severely depressed, the less psychologically minded you were,” said Dr. Roose.
Can a clinician really be effective in giving two therapies? In Dr. Roose's opinion, it can be difficult to do both adequately, because one of the two therapies is usually viewed as an adjunctive treatment by the clinician. “There is a hierarchy of treatments… whenever we have a concept of one thing being adjunctive to another, or in our own minds one thing being superior to another, I think we don't utilize the second treatment optimally,” concluded Dr. Roose.
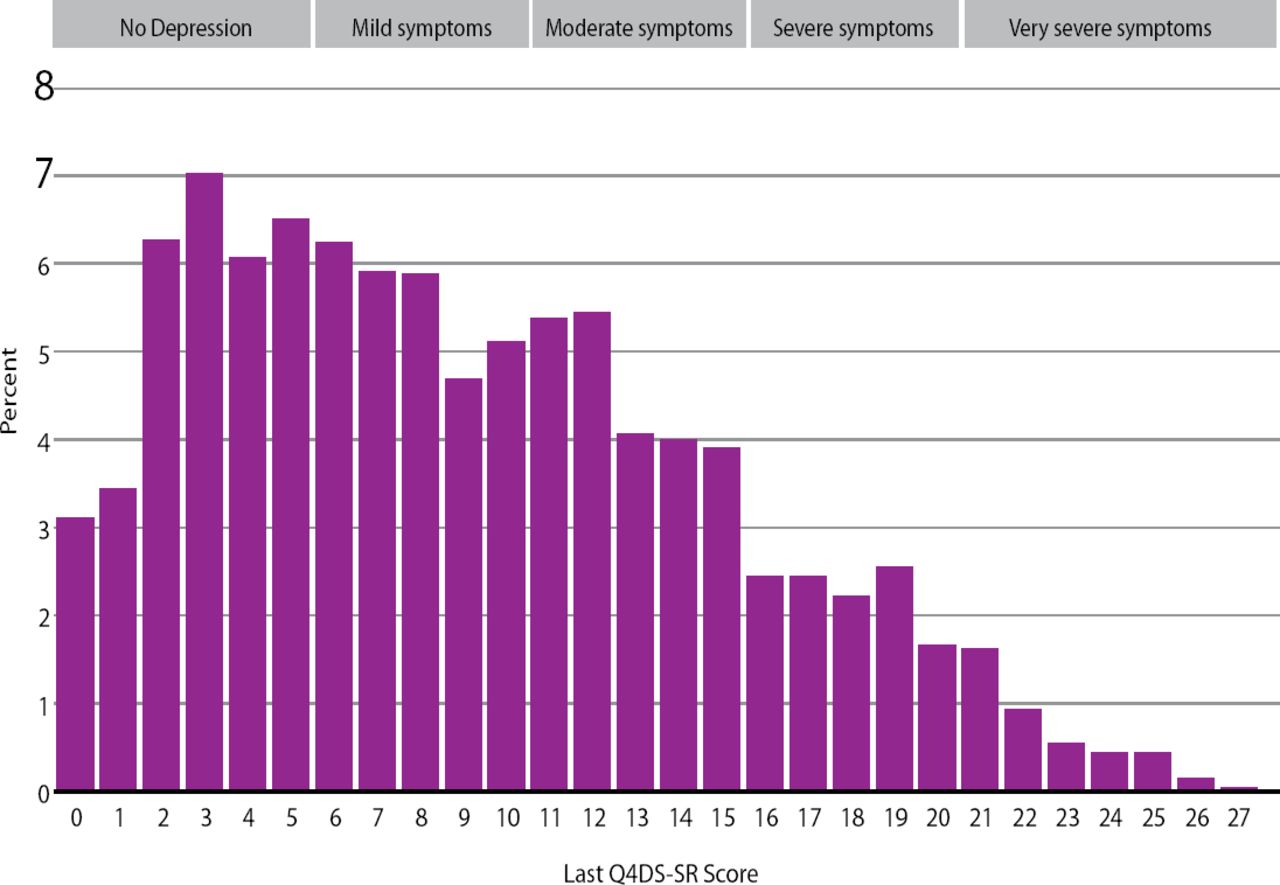
Michael Thase, MD, University of Pennsylvania, presented reasons to support further studies of combined treatment. As observed in the Sequenced Treatments to Relieve Depression (STAR-D) trial, patients with depression treated with antidepressants continue to experience residual symptoms (Figure 1; STAR*D Study Team. Am J Psychiatry 2006;163(1):28–40). For many reasons, many patients do not adhere to their pharmacotherapy, possibly because antidepressant medication still has a stigma associated with it. “I don't need to tell you all about the endemic problem of nonadherence. At least 10% of our patients never fill their first prescription, and a third don't refill the initial prescription. Thoughts and feelings about ‘Should I take this medicine? Should I keep taking it? Why am I enduring these side effects?’ are a major factor – the treatment fails,” said Dr. Thase.
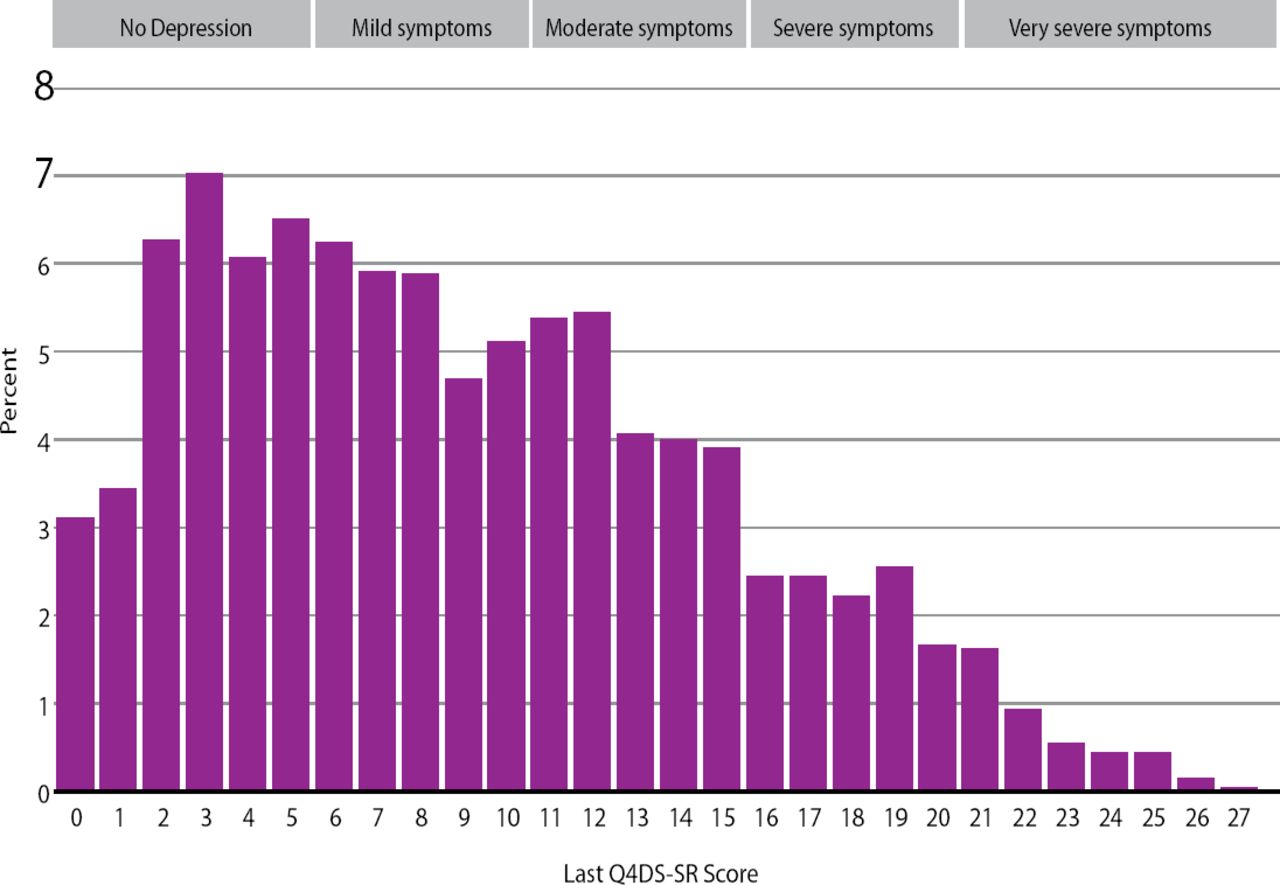
Total Exit Scores on the 16-Item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR), of 2,876 Outpatients with Nonpsychotic Major Depressive Disorder.
Because of these issues, the APA recommends combined treatment in its practice guideline for major depressive disorder. Co-administration of pharmacotherapy and psychotherapy has bidirectional effects that could ultimately reduce the potential of relapse or recurrence of depressive symptoms. The addition of psychotherapy to pharmacotherapy can improve adherence to medications, develop coping mechanisms, enhance the patient's social network and increase problem solving skills. Adding pharmacotherapy to psychotherapy can decrease limbic activation, increase a patient's capacity for enjoyment, alleviate sleep problems, improve prefrontal cortex functioning, and dampen hypothalamic-pituitary adrenal system activity.
The two types of psychotherapy that Dr. Thase discussed were interpersonal psychotherapy (IPT) and cognitive behavioral therapy (CBT). IPT is a short-term focused therapy that seeks to elucidate how interactions between people affect psychiatric symptoms. CBT instead concentrates on how a patient's internal thoughts influence personal relationships and psychiatric symptoms, with the goal of thought pattern modification. IPT has some advantages over CBT in that it may be easier for clinicians to learn. Focused therapies such as IPT and CBT have some advantages over psychodynamic psychotherapy in that they are focused on the present time, very structured, time limited, practical, personally relevant, reproducible, and can give a patient immediate hope. “I think sometimes inherent in these models of therapy is that they may better fit what people are looking for, what they believe their problems are related to. People often walk out of the first session with a little buzz, with a little sense of ‘this matches what's wrong with me, this works for me,” added Dr. Thase.
There are some impediments to researching combined therapy. Small effect sizes means larger samples sizes are needed for these types of trials, and Dr. Thase echoed Dr. Roose's observation that allegiances to therapies can obscure research findings. “This is not a mission impossible. If you're doing a study of IPT and CBT, you just need to be sure that IPT is done with the same enthusiasm…as CBT,” commented Dr. Thase. Patients perceive which therapy their doctors prefer, and will react accordingly.
“At this moment in time we cannot assertively demand from those who fund health care that combined treatment be made available to the patients who have the most difficult to treat mood disorders,” concluded Dr. Thase. Studies that are statistically powered to demonstrate a treatment difference and conducted in an appropriate non-biased manner are truly needed.
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.