

Summary
Despite an initial description of resistance to antiplatelet therapy more than 50 years ago, this concept continues to be controversial because of the lack of a widely accepted definition, method of measurement, and approach to management. For the sake of clarity, we have decided to use the terms failure of therapy to indicate patients who have recurrent events despite treatment with an antiplatelet, and to limit the term resistance to those patients for whom the antiplatelet agent does not achieve its pharmacological effect, as proposed by Wiviott, et al [Circ 2004;109;3064–7].
- Coronary Artery Disease
- Thrombotic Disorders

Despite an initial description of resistance to antiplatelet therapy more than 50 years ago, this concept continues to be controversial because of the lack of a widely accepted definition, method of measurement, and approach to management. For the sake of clarity, we have decided to use the terms failure of therapy to indicate patients who have recurrent events despite treatment with an antiplatelet, and to limit the term resistance to those patients for whom the antiplatelet agent does not achieve its pharmacological effect, as proposed by Wiviott, et al (Circ. 2004;109;3064–7).
As many as 5% to 10% of patients are resistant to aspirin, according to Steven R. Steinhubl, MD, University of Kentucky, Lexington. Aspirin-resistant patients with stable coronary artery disease (CAD) have been shown to have a five-fold increased risk of death in 2 years (JACC. 2003;41:961–5), however, there is no evidence yet to suggest that altering antiplatelet therapy based on the results of subnormal platelet function test results impacts clinical outcomes.
There is significant individual variability in platelet response to clopidogrel as well, with an increased risk of treatment failure (recurrent adverse cardiovascular events, thrombotic complications, and periprocedural myocardial damage during percutaneous coronary intervention [PCI]) in patients with clopidogrel resistance.
Adnan Kastrati, MD, Deutsches Herzzentrum, Munich, Germany, noted that in the EXCELSIOR study (Impact of Extent of Clopidogrel-Induced Platelet Inhibition During Elective Stent Implantation on Clinical Event Rate) (JACC. 2006;48:1742–1750) of 802 patients evaluated for clopidogrel response prior to elective PCI, those in the highest quartile of platelet reactivity had a four-fold greater occurrence of major adverse cardiac events (MACE) at 30 days.
Overcoming Clopidogrel Resistance
Increasing clopidogrel loading from 300 mg to 600 mg (although not from 600 mg to 900 mg) and increasing the maintenance dose to 150 mg/day can significantly improve platelet response, according to studies such as the ISAR-CHOICE 2 trial (Eur Heart J. 2007;0:ehl489v1–6. Published online Feb 1, 2007). “We can get better response in platelet aggregation, but we don't know if this is clinically relevant,” concluded Dr. Kastrati.
Eric R. Bates, MD, University of Michigan, Ann Arbor, observed that increasing clopidogrel loading to 600 mg achieves a “faster, better response with fewer nonresponders,” but added that enhancement of chronic dosing may be more important. Among diabetics in the OPTIMUS trial (Optimizing Antiplatelet Therapy in Diabetes Mellitus) (Circulation. 2007;115:708), 150 mg/day dosing improved platelet inhibition in 60% of nonresponders, although 40% still had inadequate inhibition (Aggmax ≥50%).
Should We Test for Platelet Function?
Alan D. Michelson, MD, University of Massachusetts Medical School, Boston, agreed that the routine use of platelet testing is not currently indicated. Before it can be recommended, changes to therapy based on laboratory testing of aspirin resistance must be linked to improved clinical outcomes. The same holds true for clopidogrel, he said.
Nevertheless, the 2005 ACC/AHA/SCAI Guideline Update for PCI (www.acc.org) recommends that for patients in whom subacute stent thrombosis may be catastrophic or lethal, platelet aggregation studies may be considered. In this case, if <50% inhibition of platelet aggregation is demonstrated, then the maintenance dose of clopidogrel should be increased from 75 mg to 150 mg per day.
The Dually Resistant Patient
Neal Kleiman, MD, Weill Medical College of Cornell University, New York, asked, “Does clopidogrel ‘rescue’ patients who are aspirin-resistant or are many patients resistant to both drugs?” In one of the few studies to address this question, 9 patients with peripheral artery disease and aspirin resistance were given clopidogrel for 2 weeks, which rendered 6 patients aspirin-sensitive (Thromb Haemost. 2006;65:1042–3).
Dr. Kleiman's group evaluated 150 elective PCI patients for platelet aggregation and platelet activation by rapid platelet function assay; 24% were resistant to clopidogrel and 13% were resistant to aspirin (JACC. 2006;47:27–33). Nearly 50% of the aspirin-resistant patients were also resistant to clopidogrel, versus 20% of the aspirin-sensitive patients (p=.02). Most dual resistance was seen in women and in diabetics; dually resistant patients had more frequent increases in CKMB enzymes.
“The findings suggest that 10% to 15% of the elective PCI population will have aspirin resistance and about half of these patients will also be resistant to clopidogrel,” Dr. Kleiman said. “The meaning of this is unclear, but if you are concerned that your patient is not covered with aspirin, realize that they may not be covered with clopidogrel either. This makes a strong case for platelet function testing in some patients.”
Novel Antiplatelet Agents
Novel antiplatelet agents in late-stage clinical testing appear to have advantages over clopidogrel and aspirin. The top three candidates – prasugrel, cangrelor, and AZD 6140 – all have a rapid onset of action, produce a high level of inhibition, and are not associated with resistance; cangrelor and AZD 6140 are also rapidly reversible, said Dominisk J. Angiolillo, MD, University of Florida, Jacksonville.
“So far, we see excellent degrees of platelet inhibition. We need to gather clinical experience to determine if more potent inhibition will be associated with better clinical outcomes,” he said.
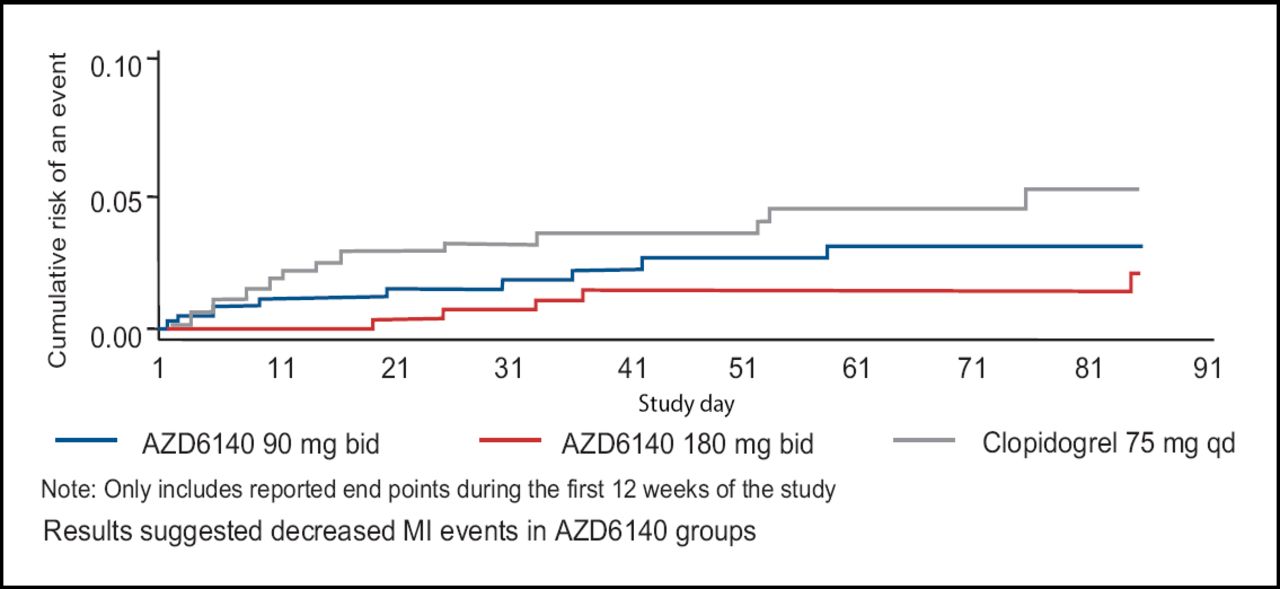
Stephen D. Wiviott, MD, Harvard Medical School, Boston, added that with prasugrel, less interpatient variability and higher concentrations in the blood result in higher, more rapid platelet inhibition. AZD 6140 has demonstrated greater platelet inhibition than clopidogrel at multiple doses, which possibly relates to a reduced risk for MI (Figure 1).

DISPERSE2. Cumulative Adjudicated Clinical End Point of MI Events.
The safety and efficacy of these agents are being evaluated in phase 3 trials that compare them to clopidogrel.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.