

Summary
Atrial fibrillation (AF) is the most common arrhythmia, yet its etiology is still not completely understood. It is becoming clear, however, that the mechanisms involved in recent onset AF may not be identical to those occurring later in the course of AF. Thus patients' treatment needs vary.
- Arrhythmias
Current Recommendations and Emerging Topics in Atrial Fibrillations
Atrial fibrillation (AF) is the most common arrhythmia, yet its etiology is still not completely understood. It is becoming clear, however, that the mechanisms involved in recent onset AF may not be identical to those occurring later in the course of AF. Thus patients' treatment needs vary. Current recommendations and emerging treatments for AF were the subjects of a number of ACC presentations.

Emerging Mechanistic Models
Miguel Valderrabano, MD, of the Methodist DeBakey Heart Center, Houston, Texas, noted that the issue of reentry is still controversial, that fibrillatory conduction is anatomically determined, and that reentry and focal discharges coexist. Multiple “self-perpetuating wavelets” have a role in the new model underlying AF, he said.
In the new “integrating” paradigm, global atrial activation patterns seem to be generated by rapid, organized activations in the left atrium, fibrillatory conduction, and frequency breakdown. Focal activity may initiate and reinitiate reentry. Pulmonary veins and the adjacent left atrium play a key role as a source of focal activations and as sites of anisotropic reentry. Additionally, the autonomic nervous system may be involved in that cholinergic influences enhance reentry and fibrillatory conduction, and sympathetic-parasympathetic interactions enhance focal discharges, he said.
Ventricular Rate Control
A. John Camm, MD, of the University of London, United Kingdom, said that control of ventricular rate can be as effective as rhythm control (restoration and maintenance of sinus rhythm) in patients with paroxysmal or persistent AF and may be even preferred in asymptomatic, sedentary, or elderly patients. Beta blockade and calcium antagonism are the main therapies for rate control. Digoxin is useful in combination, in patients with heart failure, or in sedentary patients. Amiodarone may be used intravenously or orally when other therapies for rate control are not successful, and AV nodal ablation is applicable when other therapies fail. The appropriate heart rates for optimal symptom control and outcome have not yet been established with certainty.
Radiofrequency Catheter Ablation
Most patients with AF tend to develop persistent disease with progressive substrate modification due to left atrial enlargement. While anti-arrhythmic drugs (AAD) such as amiodarone are effective in the early stage, most patients become unresponsive or develop side effects that lead to discontinuations in one third of patients later in follow-up, said Carlo Pappone, MD, PhD, of San Raffaele University Hospital, Milan, Italy.
“Unfortunately, 60% of patients have chronic AF and there is no chance to be cured without ablation,” he said.
Current guidelines for chronic AF suggest that catheter ablation be considered to maintain sinus rhythm in selected patients who fail to respond to AADs. The goals of AF ablation include pulmonary vein isolation, substrate modification, vagal denervation, and inability to induce AF or atrial tachycardia (AT), he said.
In Dr. Pappone's experience in over 14,000 patients, 87% achieve freedom from AF with ablation compared with 22% treated with amiodarone. Multiple studies have found ablation to be superior to drugs, he said, “whether patients are treated after an initial episode or after a long history of paroxysmal disease.”
Since the mechanisms of chronic AF are more complex than those causing paroxysmal AF, more extensive procedures that modify the electrical substrate as well as the initiators of AF are often necessary to prevent chronic disease. A stepwise, tailored approach to “de-complexing the AF,” substrate modification has rendered 90% of his patients free of AF at 1 year. He predicted that, in the future, clinicians will be able to construct a limited ablation procedure that targets the mechanisms unique to the individual and thus preserve the left atrium and prevent progression. Another promising treatment discussed by Ralph J. Damiano, MD, of Washington University School of Medicine, St. Louis, involves a minimally invasive surgical approach (simplified version of the Maze III procedure) that utilizes linear lines of transmural ablation that replicates the full lesions of the surgical incisions.
Emerging AAD Compounds
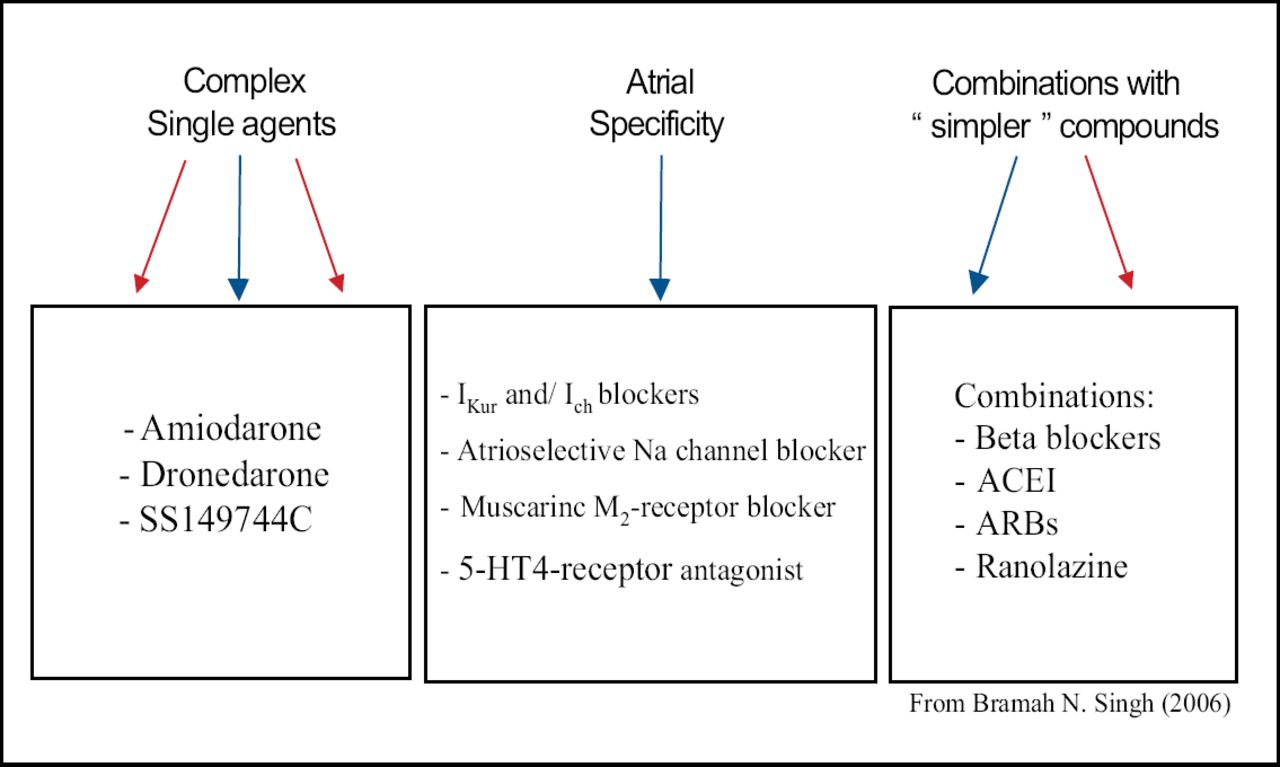
Bramah N. Singh, MD, of the David Geffen School of Medicine, University of California, Los Angeles, said sinus rhythm should be the goal “for all patients in whom conversion and maintenance of sinus rhythm is possible.” Drug development is aimed at this goal, with the major focus being two distinct categories of agents: 1) complex agents, specifically the de-iodinated amiodarone congeners dronedarone and SSR 149744C, and 2) simpler agents, ie, atrial-specific agents, such as RSD 1235 (Cardiome), a novel amino cyclohexyl ether drug with a unique Na ion channel blocking profile (Figure 1).

Augmenting Maintenance of Sinus Rhythm in Atrial Fibrillation by Antiarrhythmic Combinations – the Way of the Future?
Dr. Pappone emphasized the need to individualize treatment. “No approach will be successful in 100% of patients.”
In addition, patients should be counseled that repeat procedures may be required, particularly if there is recurrent pulmonary vein conduction, left atrial enlargement, or easy induced AF, said G. Neal Kay, MD, University of Alabama, Birmingham. Fortunately, the success of ablation is higher after repeat procedures and patients should be told to expect a second or third procedure to achieve long-term success.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.