

Summary
Percutaneous coronary intervention (PCI) is a widely used method of restoring normal blood flow to the myocardium and is lifesaving during acute coronary events. There are little long-term clinical outcome data, however, on the benefits of PCI in patients who have stable coronary artery disease. This article discusses the results of the Clinical Outcomes Utilizing Revascularization and Aggressive Guideline-Driven Drug Evaluation study [COURAGE; N Engl J Med 2007; 356:1503–1516].
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Coronary Artery Disease
Percutaneous coronary intervention (PCI) is a widely used method of restoring normal blood flow to the myocardium and is lifesaving during acute coronary events. There are little long-term clinical outcome data, however, on the benefits of PCI in patients who have stable coronary artery disease (CAD). William E. Boden, MD, of the Western New York Veterans Affairs Healthcare Network presented the results of the Clinical Outcomes Utilizing Revascularization and Aggressive Guideline-Driven Drug Evaluation (COURAGE) study (N Engl J Med. 2007; 356:1503–1516). The objective of this study was to determine if PCI combined with optimal medical therapy (OMT) was more beneficial than optimal medical therapy alone in patients with stable coronary artery disease. The primary endpoint was death from any cause or nonfatal myocardial infarction (MI) during a median follow-up period of 4.6 years.
The study was conducted from 1999 to 2004 at 50 sites in the United States and Canada. Patients with myocardial ischemia and significant CAD were randomly assigned to either PCI with OMT (n=1,149) or OMT alone (n=1,138). OMT was defined as the best pharmacological treatment possible including medications such as aspirin, beta-blockers, statins (target LDL-C of 60 to 85 mg/dL), HDL-C raising therapies if required, and ACE inhibitors plus therapeutic lifestyle changes such as weight loss, improved diet, exercise, and smoking cessation. PCI was attempted in 1,007 patients; 1,006 received at least one stent. It is important to note that this study evaluated bare metal stents, as drug-coated stents were not yet available.
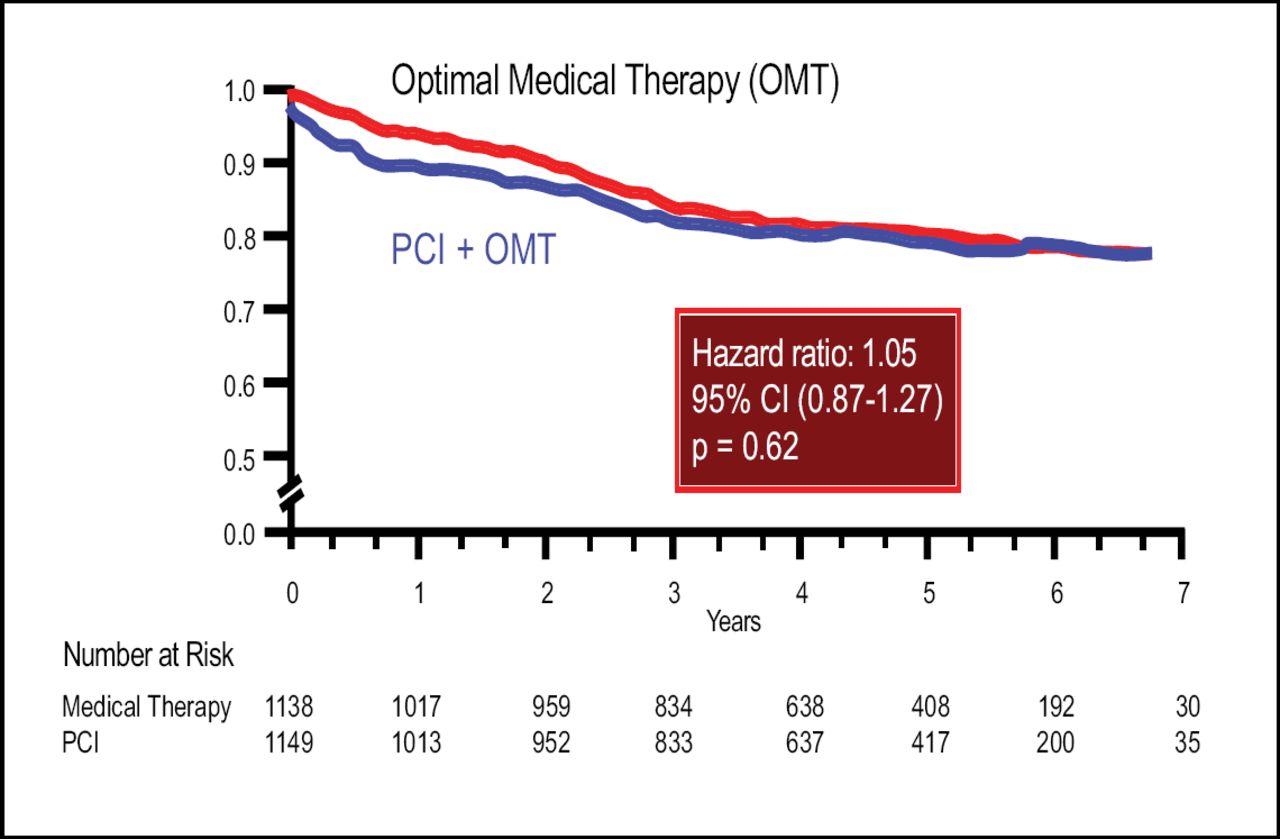
During follow-up, no differences were observed in the primary endpoint (HR=1.05; 95% CI, 0.87 to 1.27). Results were virtually identical for the secondary endpoint death, MI, and stroke (HR=1.05; 95% CI, 0.87 to 1.27; Figure 1). Additional analyses also indicated no differences in acute coronary syndrome hospitalizations (hazard ratio=1.07; 95% CI, 0.84 to 1.37) or MI (HR=1.13; 95% CI, 0.89 to 1.43). A similar number of patients required subsequent coronary artery bypass grafts (77 in the PCI group; 81 in the OMT group). Subgroup analyses did not reveal any interactions between the treatment effect and defined variables such as age, sex, or diabetes.

Survival Free of Death from Any Cause and Myocardial Infarction.
William S. Weintraub, MD, of the Christiana Healthcare System, Wilmington, Delaware gave a brief overview of the health status and economic outcomes data from the COURAGE study. Quality of life data was gathered by administering surveys including the Seattle Angina Questionnaire, the Rand 36, and the Utility by Gamble, at baseline, 1, 3, 6, and 12 months after randomization, and annually thereafter. The investigators found that angina improved in both treatment arms although the PCI group had a slight but significant incremental benefit compared to OMT. However, PCI was a more expensive choice for patients with stable CAD.
The authors concluded that the results of this study confirm the current American College of Cardiology/American Heart Association clinical practice guidelines that state that PCI may be deferred in stable patients as long as OMT is initiated.
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.