

Summary
Menopause-associated bone loss begins during perimenopause, ∼?2 years before the last menstrual period. This article presents data from the Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Effects of Alendronate on Bone Mineral Density and Bone Turnover in Perimenopausal Women With Low BMD poster [ICE/ENDO 2014. Poster LBSA-0269], first study to evaluate the efficacy of an antiresorptive agent on maintaining BMD in perimenopausal women.
- metabolic bone disease
- menopause
- diabetes & endocrinology clinical trials
Alendronate plus cholecalciferol treatment improved bone mineral density (BMD) at the lumbar spine and reduced bone turnover in perimenopausal women with low BMD. Aliya Khan, MD, McMaster University, Hamilton, Ontario, Canada, presented data in a poster from the Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Effects of Alendronate (ALN) on Bone Mineral Density (BMD) and Bone Turnover in Perimenopausal Women With Low BMD [ICE/ENDO 2014. Poster LBSA-0269].
Menopause-associated bone loss begins during perimenopause, ∼ 2 years before the last menstrual period. The purpose of this study was to determine if treatment with alendronate (ALN), an antiresorptive agent, can prevent bone loss in women who are perimenopausal and have low BMD. This is the first study to evaluate the efficacy of an antiresorptive agent on maintaining BMD in perimenopausal women.
In this double-blind trial, women aged 40 to 55 years with reduced bone density (T-score < −1.0) of the lumbar spine, total hip, or femoral neck were randomly assigned to receive 70 mg of ALN plus 2800 IU of cholecalciferol (vitamin D3) once weekly or placebo for 1 year. In addition, all patients received 500 mg of calcium carbonate once daily. Patients were eligible if they had at least 5 menstrual periods per year and had follicle-stimulating hormone (FSH) levels > 20 IU/L but < 40 IU/L on 2 independent occasions. Patients were excluded if they had hyperthyroidism, hyperparathyroidism, liver disease, acromegaly, Cushing syndrome, rheumatoid arthritis, myeloma, Paget disease, renal osteodystrophy, osteomalacia, or polycystic ovarian disease. Other exclusion criteria included treatment during the past 6 months with androgens, calcitonin, systemic corticosteroids, fluoride, parathyroid hormone, selective estrogen receptor modulators, estrogen, oral contraceptives, bisphosphates, vitamin D > 2000 IU per day, or vitamin D metabolites. In addition, patients with esophageal abnormalities, including stricture or achalasia, were excluded from the study.
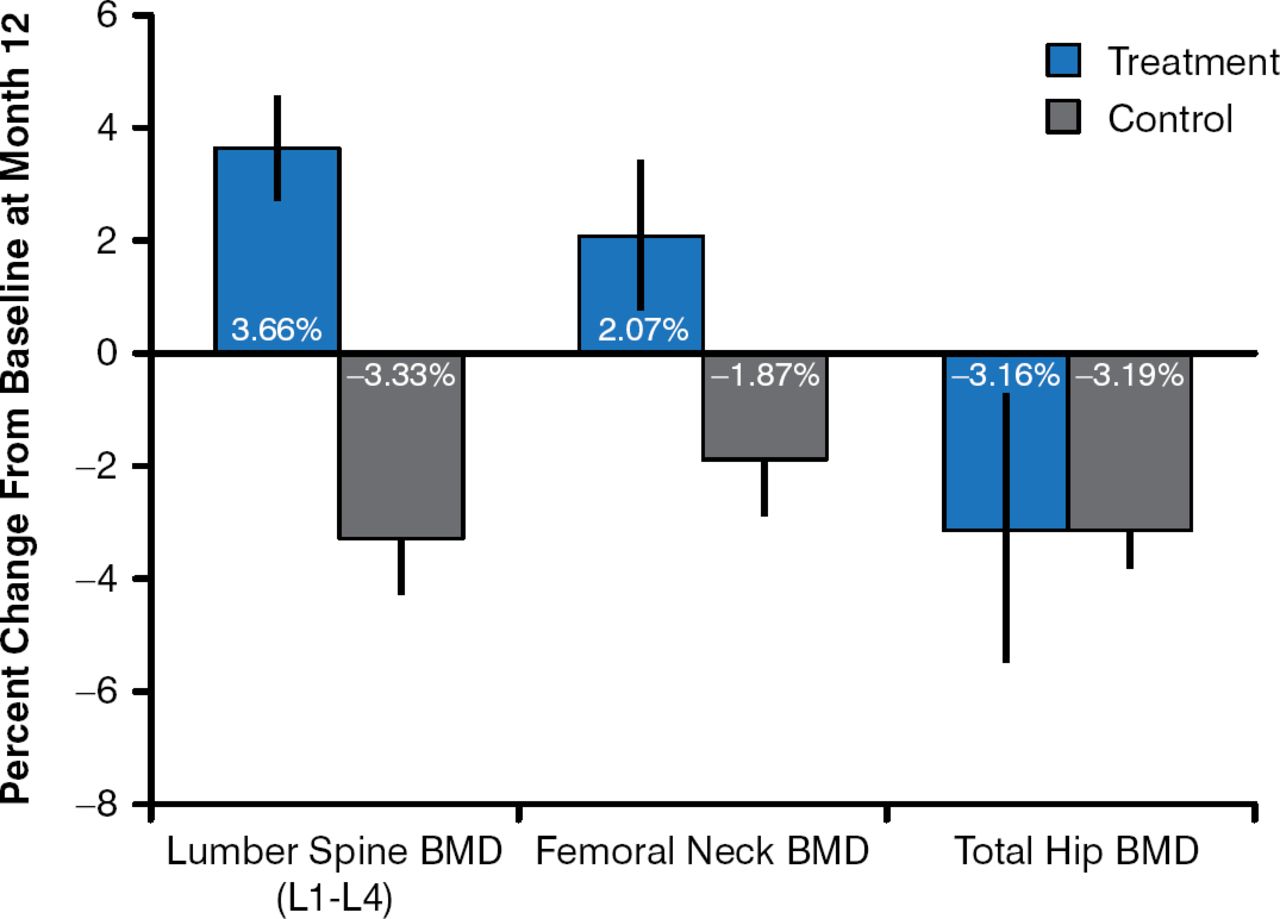
At 12 months, there was a significant increase in BMD at the lumbar spine (L1 to L4; 3.66%; p < .01) and a trend of increased BMD at the femoral neck (2.07%; p = .14) from baseline among patients who received ALN plus cholecalciferol compared with placebo (Figure 1). In addition, there was a significant decrease in bone-specific alkaline phosphatase (−37.8%; p < .01) and N-telopeptide in the urine (27.2%; p = .03) and an increase in FSH (101.13%; p < .01), as well as a trend of decreased N-telopeptide in the serum (−27.6%; p = .23), from baseline in the ALN arm compared with the placebo arm. Treatment with ALN plus cholecalciferol resulted in no significant difference from baseline compared with placebo in albumin, calcium, phosphate, magnesium, estradiol, or urine creatinine.

Effect of Alendronate on BMD in Perimenopausal Women
BMD=bone mineral density.
Reproduced with permission from A Khan, MD.
In conclusion, treatment of perimenopausal women with low BMD with ALN plus cholecalciferol reduced bone turnover and improved BMD in the lumbar spine over 12 months. Prof. Khan indicated that the data from this study suggest that providing early intervention with a bisphosphonate during the menopausal transition may limit BMD loss.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.