

Summary
The Diabetes Attitudes Wishes and Needs 2 study [DAWN2; Peyrot M et al. Diabetes Res Clin Pract 2013], with more than 16,000 participants, has reaffirmed the need to improve the self-management of type 1 diabetes mellitus (T1DM) or type 2 diabetes mellitus (T2DM) and revealed the extent of diabetes-related distress among those with diabetes and their families. Better psychosocial and behavioral outcomes are linked to the availability of a strong social support network. This article discusses the findings and implications of DAWN2.
- Diabetes Mellitus
- Prevention & Screening Diabetes & Metabolic Syndrome
- Nursing
- Diabetes Mellitus
- Prevention & Screening
- Endocrinology
- Diabetes & Metabolic Syndrome
- Nursing
The Diabetes Attitudes Wishes and Needs 2 study [DAWN2; Peyrot M et al. Diabetes Res Clin Pract 2013], with more than 16,000 participants, has reaffirmed the need to improve the self-management of type 1 diabetes mellitus (T1DM) or type 2 diabetes mellitus (T2DM) and revealed the extent of diabetes-related distress among those with diabetes and their families. Better psychosocial and behavioral outcomes are linked to the availability of a strong social support network. Martha M. Funnell, MS, RN, CDE, FAADE, University of Michigan Medical School, Ann Arbor, Michigan, USA, discussed the findings and implications of DAWN2 in a keynote address.
DAWN2 built on the data from the 2001 DAWN study [Skovlund SE et al. Diabetes Spectr 2005], conducted with more than 5000 adults with T1DM or T2DM and with almost 4000 health care providers (HCPs) across 13 countries. DAWN revealed the less-than-optimal self-management of diabetes, which was largely driven by widespread but untreated psychosocial problems (85% reported severe distress at diagnosis; 43% at mean 15 years).
According to the International Diabetes Foundation, people living with diabetes will increase from 382 million adults in 2013 to an estimated 592 million by approximately 2030 [International Diabetes Federation. IDF Diabetes Atlas. 6th ed. 2013]. Primary health care systems are already struggling to provide preventive and chronic care for diabetes. Having family members assume a more active role can ease the health care burden and allow those directly affected by diabetes to take a proactive role in their health.
As diabetes becomes more widespread, HCPs must play a bigger role in improving quality of life (QoL) and outcomes for people with diabetes, according to Funnell. Although DAWN solicited input from HCPs and adults with diabetes, DAWN2 also included responses from family members of adults with diabetes.
The primary objective of DAWN2 was to assess potential obstacles and drivers of successful diabetes management by people with diabetes, family members, and HCPs [Peyrot M et al. Diabetes Res Clin Pract 2013]. Secondary objectives included the following: setting national benchmarks for health, QoL, and access to diabetes self-management education and self-care; assessing availability and benefit of HCPs, family members, and other caregivers; identifying the aids and barriers to self-managed chronic care; and evaluating what is presently working and what needs to be changed in diabetes care.
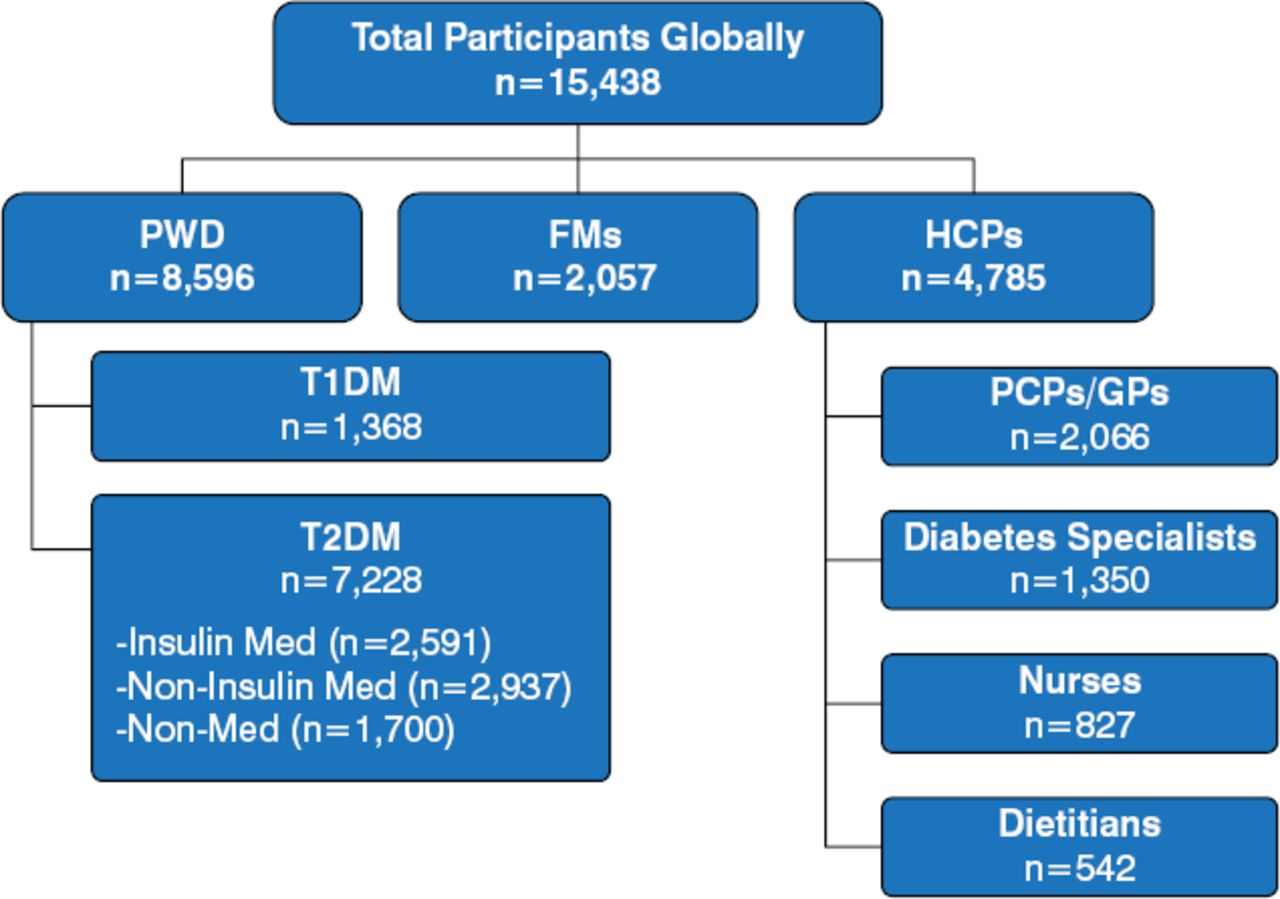
DAWN2, an interdisciplinary and multistakeholder study, enrolled 15 438 participants from 17 countries over 4 continents between March 2012 and August 2012. The total study population comprised 8596 persons with diabetes (T1DM, n=1368; T2DM, n=7228), 2057 family members, and 4785 HCPs, comprising primary care physicians, general practitioners, diabetes specialists, nurses, and dietitians [Holt RIG et al. Diabet Med 2013; Kovacs Burns K et al. Diabet Med 2013; Nicolucci A et al. Diabet Med 2013].
Participants completed a questionnaire regarding demographics, health and QoL, diabetes training, diabetes profile, active self-management, attitudes and beliefs about diabetes, care and support/involvement, diabetes education and information, and future needs [Peyrot M et al. Diabetes Res Clin Pract 2013]. A separate qualitative analysis was conducted to further explain the successes, wishes, and needs for improvement in diabetes management [Stuckey H et al. Diabetes Care 2014).
Among people with diabetes, 45% experienced diabetes-related emotional distress, with 14% reporting feelings of depression [Nicolucci A et al. Diabet Med 2013]. The roots of the distress varied and included reduced physical health (62%), diminished emotional well-being (46%), financial burden (44%), restricted leisure activities (38%), detrimental effect of work or study (35%), and strained relationships with family, friends, and others (21%). Only one-quarter of adults with diabetes indicated that their HCPs asked how diabetes affected their lives, while 52% of HCPs reported asking about the issue during a visit [Holt RIG et al. Diabet Med 2013]. Forty percent of family members reported experiencing substantial diabetes-related distress, with 35% reporting a moderate to very high burden of care [Kovacs Burns K et al. Diabet Med 2013]. Family members also reported reduced emotional well-being (45%), financial hardship (35%), fewer leisure activities (31%), diminished physical health (27%), work/study challenges (23%), and difficulties in relationships (family, friends, peers; 20%). Despite these challenges, family members wanted to assist more in helping their relatives cope with diabetes-related distress (46%) and in care (39%), but 37% did not know how best to do so. The majority of HCPs (85%) wanted people with diabetes to better communicate with their HCPs on how they can help. Of the HCPs, 60% felt that more self-management education was needed and would lessen the disease burden [Holt RIG et al. Diabet Med 2013].

The DAWN2 Total Study Population
FMs=family members; GPs=general practitioners; HCPs=health care providers; PCPs=primary care physicians; PWD=persons with diabetes; T1DM=type 1 diabetes mellitus; T2DM=type 2 diabetes mellitus.
Reproduced with permission from MM. Funnell, MS, RN.
Less than half of the surveyed adults with diabetes and 23% of family members participated in the study designed to help in diabetes management [Kovacs Burns K et al. Diabet Med 2013; Nicolucci A et al. Diabet Med 2013]. The majority of patients and family members (81% and 72%, respectively) found the management information helpful. Yet, relatively few said that they were asked how chronic diabetes affected their lives and whether they felt anxious or depressed in the prior 12 months (24% and 32%, respectively). Results from DAWN2 also suggest that diabetes was linked to considerable psychosocial challenges, and discrimination due to diabetes is prevalent, owing to a lack of education and awareness (Table 1).
Key DAWN2 Findings
The US arm of DAWN2 had 940 participants (539 people with diabetes, 121 family members, and 280 HCPs). Of these, 799 were African Americans, Hispanics, and Chinese Americans (537 people with diabetes, 122 family members, and 140 HCPs). Self-management varied among the 3 minorities (Table 2).
Self-management Behaviors Among Ethnicities in DAWN2a
Ethnic differences were also evident concerning psychological well-being, with non-Hispanic whites faring worse than African Americans, Hispanics, and Chinese Americans in scores of well-being, QoL, diabetes empowerment, impact of diabetes. However, all ethnic minorities fared worse than non-Hispanic whites for diabetes-related distress. Non-Hispanic whites were also less likely to ask for support and seek out information for help in the selfmanagement of their diabetes. Of the total US participants, 64% of adults with diabetes and 35% of family members took part in diabetes educational programs and activities. Most found these helpful (78% and 70%, respectively).
The collective findings indicate that those with diabetes fare better when they seek support. Family members can be helpful, especially as listeners, but they may lack the knowledge and skills necessary for optimal support. A prudent selfmanagement program should equally consider the needs of patients and their families. According to Funnell, the most important questions for HCPs to ask people with diabetes is how it affects their lives and with what are they struggling. By helping people with diabetes identify problems and concerns rather than solely focus on their behaviors, HCPs can help patients set goals and embark on making beneficial changes with the support of their loved ones.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.