

Summary
This article discusses the value of the 8-parameter Global Registry of Acute Coronary Events (GRACE) risk score [The GRACE Investigators. Am Heart J 2001] in predicting the 1-year mortality of patients discharged with acute coronary syndrome (ACS).
- Myocardial Infarction
- Cardiology Clinical Trials
- Prevention & Screening
- Myocardial Infarction
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Prevention & Screening
Michael Chin, DM, University of the West Indies, Trinidad and Tobago, described the value of the 8-parameter Global Registry of Acute Coronary Events (GRACE) risk score [The GRACE Investigators. Am Heart J 2001] in predicting the 1-year mortality of patients discharged with acute coronary syndrome (ACS).
ACS causes about 50% of all cardiovascular-related deaths, and the 1-year survival of ACS patients depends on a variety of patient-related factors and the care received during hospitalization [Lloyd-Jones D et al. Circulation 2010]. Management of ACS patients is challenging in a resource-limited setting. Identifying patients at higher risk who may benefit from more aggressive treatment, such as early invasive strategies and coronary care unit monitoring, could help to allocate available resources in an optimal way.
Three risk scores—Thrombosis in Myocardial Infarction, Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using in Tegrilin, and GRACE—are recommended for patient stratification [de Araújo Gonsalves P et al. Eur Heart J 2005]. All, especially GRACE, have good predictive accuracy for death and myocardial infarction before discharge and up to 1 year following discharge.
The GRACE investigators previously showed the utility of the GRACE risk score in predicting in-hospital mortality (8.3% of 372 patients) in a multiethnic population in the resource-limited setting of Trinidad and Tobago. The present study analyzed follow-up data in the 341 survivors following hospital discharge to explore whether the GRACE score is valuable in predicting 1-year mortality.
The majority of the patients (n = 207 of 341) were aged > 60 years, and about 72% were of Indian ethnicity. The presenting ACS was categorized as STEMI (ST segment elevation myocardial infarction; 25.2%), non-STEMI (54.3%), and unstable angina pectoris (20.5%).
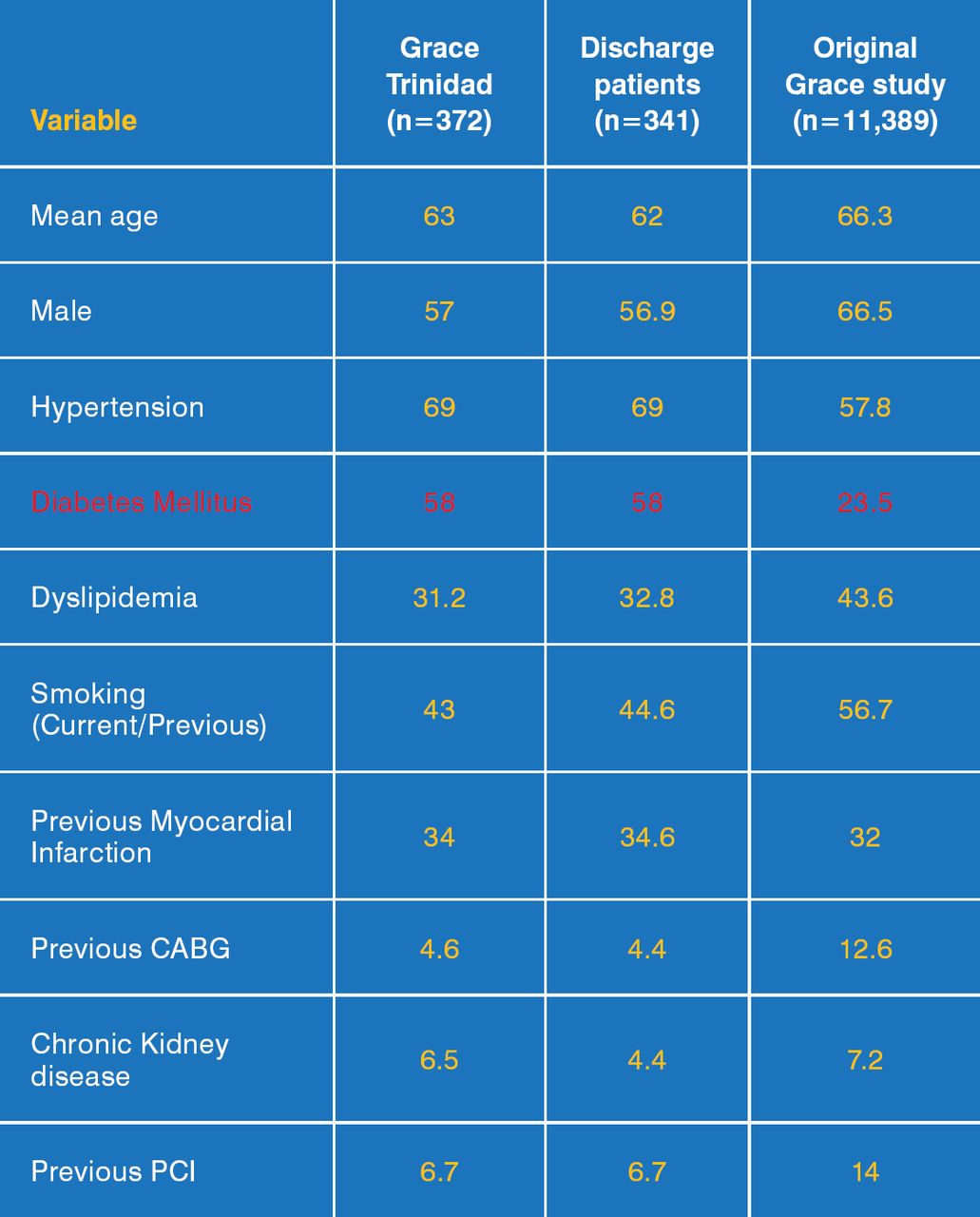
The baseline characteristics of patients in the hospitalized and discharged groups in the present study were similar, with both groups differing from the original GRACE study (which predominantly involved Caucasian patients) in terms of the prevalence of diabetes mellitus and hypertension (Figure 1).

Baseline Characteristics
CABG=coronary artery bypass grafting; PCI=percutaneous coronary infarction.
Reproduced with permission from M Chin, MD.
The GRACE risk category distribution was fairly even, with high, intermediate, and low risk constituting 30.2%, 34.9%, and 34.9% of the discharged patients, respectively. However, subjects who died were predominantly in the high-risk group (31.5%), compared with the intermediate- (8.3%) and low-risk (3.5%) groups. Predictors of 1-year mortality included age, creatinine, elevated cardiac enzymes, heart rate at admission, Killip class, history of chronic kidney disease, and the GRACE risk score.
The results of the present study extend the utility of the GRACE risk score from a predominantly Caucasian population to patients from a developing (resource-limited) country with a multiethnic population.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.