

Summary
In recent decades, the landscape for management of patients with acute coronary syndrome (ACS) has changed dramatically. This article discusses how some of these changes have significantly improved outcomes in the Swedish patient population.
- Cardiology
- Myocardial Infarction
- Interventional Techniques & Devices
- Cardiology
- Myocardial Infarction
- Interventional Techniques & Devices
In recent decades, the landscape for management of patients with acute coronary syndrome (ACS) has changed dramatically. In a State of the Art Lecture, Stefan James, MD, PhD, Uppsala University Hospital, Uppsala, Sweden, discussed how some of these changes have significantly improved outcomes in the Swedish patient population.
IMPLEMENTATION OF RESEARCH FINDINGS AND GUIDELINES
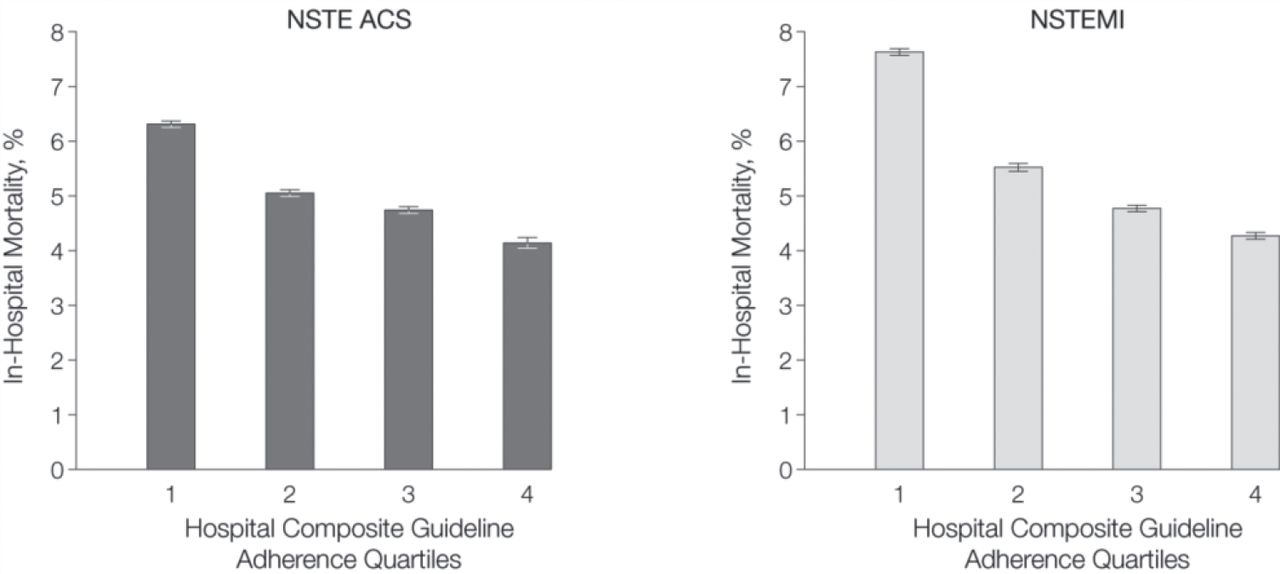
Prof James highlighted the importance of following guideline recommendations in patients with ACS, discussing results from an observational study demonstrating that every 10% increase in adherence to guideline recommendations of the American College of Cardiology and the American Heart Association results in a 10% decrease in mortality (Figure 1) [Peterson ED et al. JAMA. 2006].

Association Between Adherence to ACC and AHA Guidelines and Patient Mortality
ACC, American College of Cardiology; AHA, American Heart Association.
Every 10% increase in guidelines adherence → 11% decrease in mortality.
Reproduced from Peterson, ED. Association Between Hospital Process Performance and Outcomes Among Patients With Acute Coronary Syndromes. JAMA. 2006;295:1912–1920. Copyright © 2006 American Medical Association. All rights reserved.
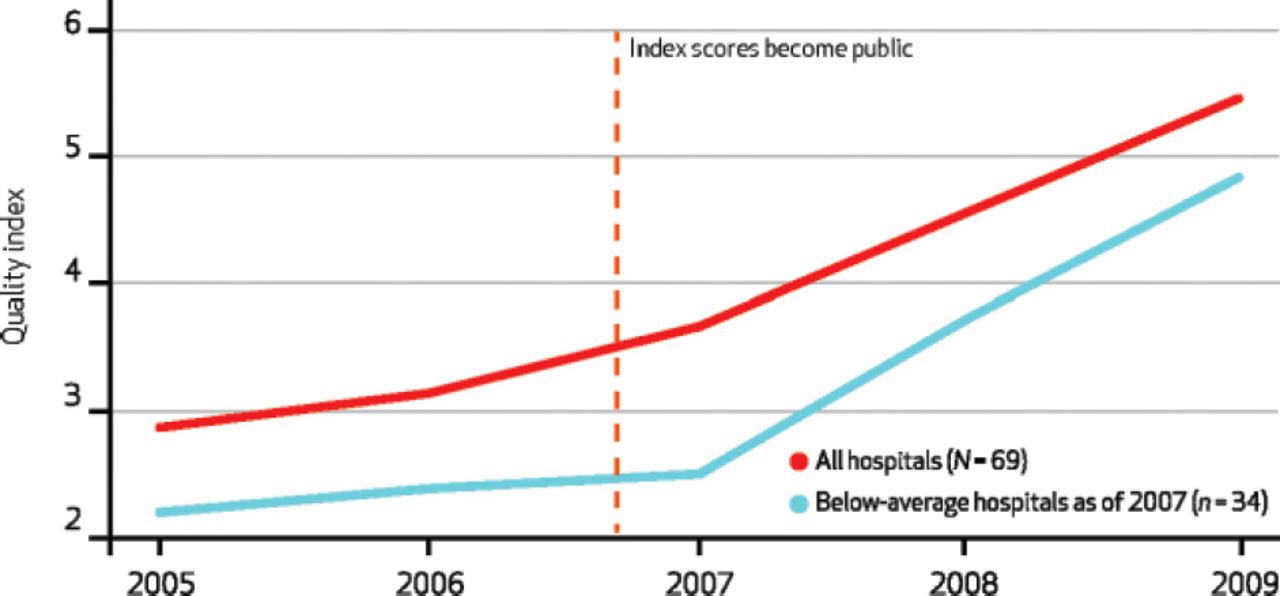
He also presented data from the SWEDEHEART registry [SWEDEHEART. Eur Heart J. 2009], Sweden's new online national cardiac registry of all patients hospitalized with ACS or undergoing coronary or valvular intervention. Following implementation of this registry, from 2005 to 2011, there was a dramatic improvement in how Swedish hospitals met guideline recommendations for the management of these patients. Prof James also noted that the rate of uptake of adherence to guidelines also markedly improved when hospitals' outcomes data were made transparent to both practitioners and the public (Figure 2) [Larsson S et al. Health Affairs. 2012]. From 1996 to 2007, increased adherence to evidence-based treatments in STEMI patients was also associated with a sharp decline in mortality from 21% to 12% [Jernberg T et al. JAMA. 2011].

Change in Adherence to Guidelines Following Public Reporting of Hospital Outcomes Data
Copyrighted and published by Project HOPE/Health Affairs as Larsson S et al. Use of 13 Disease Registries in 5 Countries Demonstrates the Potential to Use Outcome Data to Improve Health Care's Value. Health Aff. (Millwood). 2012;31:1, 220–227. The published article is archived and available online at http://healthaffairs.org.
INNOVATIVE REPERFUSION AND INTERVENTIONAL STRATEGIES
Primary percutaneous coronary intervention (PCI) was another important innovation for patients with ACS and STEMI. Prof James discussed the marked shift in the past decade from the use of fibrinolysis to PCI, and how this has been associated with a lower risk of bleeding complications and has almost completely eliminated the occurrence of fatal bleeds. This transition has also improved the delay to reperfusion and dramatically reduced the incidence of cardiogenic shock. He noted that most patients aged > 65 years are now receiving primary angiography for STEMI and primary PCI.
Another important shift is in the transition from using femoral to using radial access for primary PCI. According to Prof James, from 2003 to 2013, the number of patients receiving radial procedures increased from approximately 15% to almost 80%. Compared with femoral access, radial access is also associated with a reduction in complications during hospitalization, most notably a 50% decrease in all bleeding risk.
INTERVENTIONAL DEVICES
There has also been a significant evolution throughout time in drug-eluting stent (DES) design with regard to the drugs, polymers, stent platforms, and delivery systems involved. Old-generation DES (o-DES), despite being safe, has been associated with an increased risk of late stent thrombosis (LST) [Sarno G et al. J Am Coll Cardiol 2014]. Recent data from the SWEDEHEART study have shown that the LST risk associated with newer-generation DES (n-DES) is similar to that associated with bare-metal stents (BMS) and lower than that of o-DES.
Prof James described the introduction of bioresorbable vascular scaffolds (BVSs) as the fourth revolution in interventional cardiology. He noted, however, that observational data thus far have shown a markedly increased stent thrombosis (ST) risk using BVS technology compared with n-DES. In one study, the cumulative incidence of definite or probable scaffold thrombosis was 1.5% at 30 days and 2.1% at 6 months, with 16 of 23 cases occurring within 30 days [Capodanno D et al. Eurointervention. 2014]. So, although this new technology holds promise, Prof James emphasized the importance of optimizing the implantation technique and using intracoronary imaging to reduce the thrombosis risk throughout time.
PHARMACOLOGICAL AGENTS AND STRATEGIES
Pharmacological agents and strategies have revolutionized PCI and treatment of patients with PCI. In Sweden, secondary prevention with statin treatment has greatly increased throughout time since 1994, and now most patients receive statin treatment post ACS.
Prof James believes that potent statin therapy is one of the most important contributors to the low patient mortality post myocardial infarction (MI).
New platelet inhibitors have also emerged, including the novel P2Y12 antagonist ticagrelor, which inhibits adenosine diphosphate—induced platelet aggregation more potently than clopidogrel and reduces the incidence of MI and death in patients with ACS [Damman P et al. J Thromb Thrombolysis. 2012]. According to Prof James, since its launch in 2011, ticagrelor has now taken > 80% of the market in Sweden, with a simultaneous reduction in the use of clopidogrel down to approximately 15% of the patient population.
SECONDARY PREVENTION AND ASSESSMENT OF PATIENT-REPORTED OUTCOMES
Patients now report reductions in sick leave following MI. According to Prof James, registry data for the SWEDEHEART registry have shown that from 2006 to 2012, the number of patients working full-time 6 to 10 weeks post MI has increased from about 40% to 65% in 2012, and only 20% are now at full sick leave [Hambraeus et al. Scand Cardiovasc J. 2014].
PRIMARY AND SECONDARY PREVENTION STRATEGIES
Prof James also discussed the large, prospective, registry-based randomized TASTE trial [Lagerqvist B et al. N Engl J Med. 2014], which was conducted to determine the effect of intracoronary thrombus aspiration on distal embolization and perfusion. Patients with STEMI were randomized to receive thrombus aspiration or to not receive thrombus aspiration prior to PCI. At 1 year, the results demonstrated no significant difference between the groups in mortality (P = .57), rehospitalization for MI (P = .81), or ST (P = .48).
He remarked that another important area of study currently underway in the SWEDEHEART registry (VALIDATE) is a randomized comparison of heparin vs bivalirudin in STEMI or NSTEMI patients treated with ticagrelor or prasugrel pre-PCI. The primary outcomes are death, MI, and major bleeding events.
Thanks to innovations in pharmaceutical agents, devices, strategies, and trial design and implementation, there have been significant decreases in the morbidity and mortality of cardiovascular disease in Europe and large parts of the world [Nabel EG, Braunwald E. N Engl J Med 2012]. About half of the reduction is explained by evidence-based medical therapies in the acute phase, and about half is attributable to risk factor modification [Ford ES et al. N Engl J Med. 2007]. In his concluding remarks, however, Prof James emphasized the need for continued innovation, because ischemic heart diseases and cerebrovascular diseases are predicted to remain the 2 leading causes of death worldwide for some time to come.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.