

Summary
Results of the Comparison of FFR-guided and Angiography-guided Provisional Stenting for True Coronary Bifurcation Lesions: A Randomized, Multi-center Clinical Trial [DKCRUSH-VI] show that fractional flow reserve (FFR)-guided and angiography-guided provisional side branch stenting of true coronary bifurcation lesions are associated with similar rates of 1-year major adverse cardiac events.
- Interventional Techniques & Devices
- Coronary Artery Disease
- Radiography
- Cardiology Clinical Trials
- Imaging Modalities
- Cardiac Imaging Techniques
- Interventional Techniques & Devices
- Coronary Artery Disease
- Cardiology
- Radiography
- Cardiology Clinical Trials
- Imaging Modalities
- Cardiac Imaging Techniques
Results of the Comparison of FFR-guided and Angiography-guided Provisional Stenting for True Coronary Bifurcation Lesions: A Randomized, Multi-center Clinical Trial [DKCRUSH-VI] show that fractional flow reserve (FFR)-guided and angiography-guided provisional side branch (SB) stenting of true coronary bifurcation lesions are associated with similar rates of 1-year major adverse cardiac events (MACE). The DKCRUSH-VI trial is the first study to compare FFR-guided and angiography-guided stenting. The results were reported by Shao-Liang Chen, MD, Nanjing First Hospital, Lanzhou, China.
Angiographically guided provisional SB stenting after main vessel stenting is associated with favorable outcomes for the majority of coronary bifurcation lesions. FFR is the gold standard for the assessment of functional ischemia of a coronary lesion. The objective of DKCRUSH-VI was to compare the outcomes of FFR-guided and angiography-guided provisional SB stenting for true coronary bifurcation lesions.
The trial included 320 patients with true coronary bifurcation lesions (Medina 1,1,1, or 0,1,1), a SB ≥ 2.5 mm in diameter, and a lesion length in each branch that could be covered by 2 drug-eluting stents who were undergoing stenting with a provisional SB approach. Patients with a myocardial infarction (MI) < 1 month prior to the percutaneous coronary intervention (PCI) procedure and those with a left main disease bifurcation lesion with right coronary artery-chronic total occlusion not recanalized were ineligible for this study.
The primary end point was a composite of MACEs including cardiac death, MI, and target vessel revascularization (TVR). Secondary end points included cardiac death, MI, restenosis, stent thrombosis or target lesion revascularization (TLR), coronary artery bypass grafting (CABG), or TVR. Patients were randomly assigned 1:1 to an angiography-guided (n = 160) or an FFR-guided (n = 160) approach.
The proportions of patients with Medina 1,1,1 for the angiography and FFR groups were 86.8% and 82.5%, respectively. Baseline quantitative coronary arteriography (QCA) characteristics for the main vessel and SB were similar. Lesion length in the SB was shorter (nonsignificant) in the FFR group.
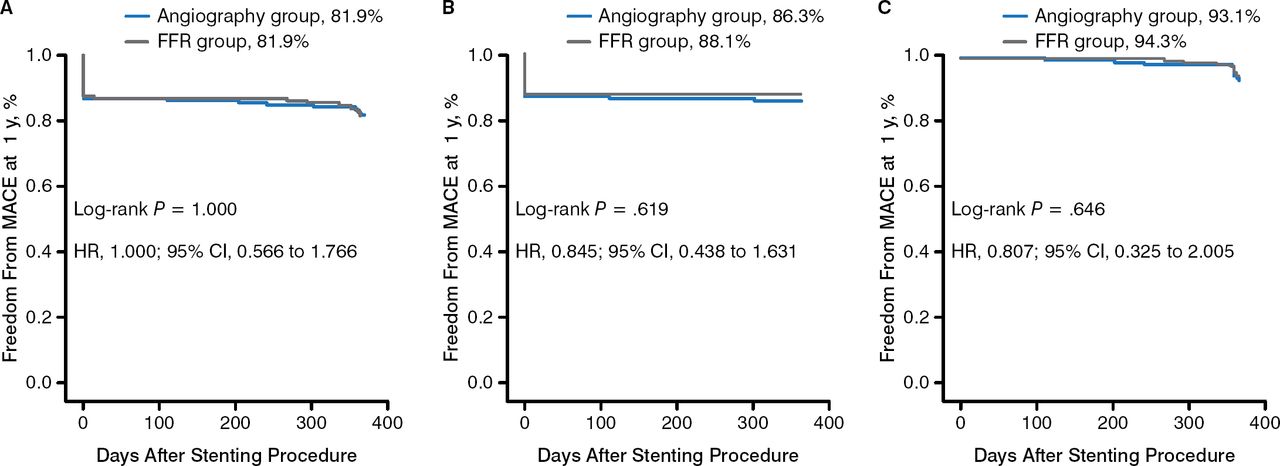
Side branch treatment (balloon or stenting) occurred in 56.3% of FFR cases vs 63.1% of angiography-guided cases (P = .07). Fewer stents were attempted in the FFR group (25.9% vs 38.1%; P = .01), but these were largely as successful as those in the angiography-guided group (77.3% vs 83.6%). There were no group differences for 1-year clinical outcomes for: cardiac death, MI, TLR, CABG, or TVR. The percentage of patients experiencing MACE was the same for both groups (18.1%). There were no significant differences in the Kaplan-Meier analysis of 1-year survival rates (Figure 1).

Kaplan-Meier Analysis for 1-Year Survival
FFR, fractional flow reserve; MACE, major adverse cardiac events; TVR, transcatheter valve replacement.
A, Composite MACE. B, Myocardial infarction. C, TVR.
Reproduced with permission from S-L Chen, MD.
In a post hoc analysis, in-segment restenosis (defined as QCA distal segment [DS] > 50%) in the distal main vessel was significantly less frequent in the FFR group (P = .01; Table 1). However, in-segment restenosis in the side branch was significantly less frequent in the angiography group (P = .037; Table 1).
Distribution of Restenosisa
Limitations of the study include the use of an arbitrary FFR cutoff of < 0.80. In addition, the small difference in MACE between the 2 approaches cannot be excluded.
Prof Chen concluded that based on the results from the current multicenter randomized trial, FFR-guided and angiography-guided provisional stenting of true coronary bifurcation lesions are associated with similar rates of 1-year MACE, but FFR-guided SB lesion stenting holds the promise of fewer stents placement.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.