

Summary
This article discusses the pathomechanics and pathoanatomy of ankle fractures, challenges involving the medial ankle ligament complex, as well as midfoot (Lisfranc) lesion closures.
- Foot & Ankle Conditions
- Trauma
- Foot & Ankle Conditions
- Orthopaedics
- Trauma
Naoki Haraguchi, MD, Johns Hopkins University, Baltimore, Maryland, USA, spoke about a new concept regarding the pathomechanics and pathoanatomy of ankle fractures. Beginning in 1948, Lauge-Hansen classified ankle fractures into 13 subgroups according to the position of the foot at the time of the fracture (supination or pronation) and the direction of the force (adduction, abduction, or external rotation). A supination-external (S-E) rotation fracture is the most common type of ankle fracture. There are clinical inconsistencies to this definition, however, and a host of different studies from the 1960s to 1990s have been unable to reproduce a Lauge-Hansen S-E rotation-type fracture in experimental settings.
Dr Haraguchi then described his group's hypothesis that an S-E rotation fracture could occur as the result of a pronation-external rotation mechanism [Haraguchi N, Armiger RS. J Bone Joint Surg Am. 2009]. In the first phase of their study, they used 15 cadaver limbs mounted onto a materials-testing machine. Putting the ankle in the pronated position, the researchers applied both axial force (100 N/s, maintained at 700 N) and an external rotation moment. In the second phase, an additional 8 specimens were tested, to which an additional external force was applied laterally to the foot carriage.
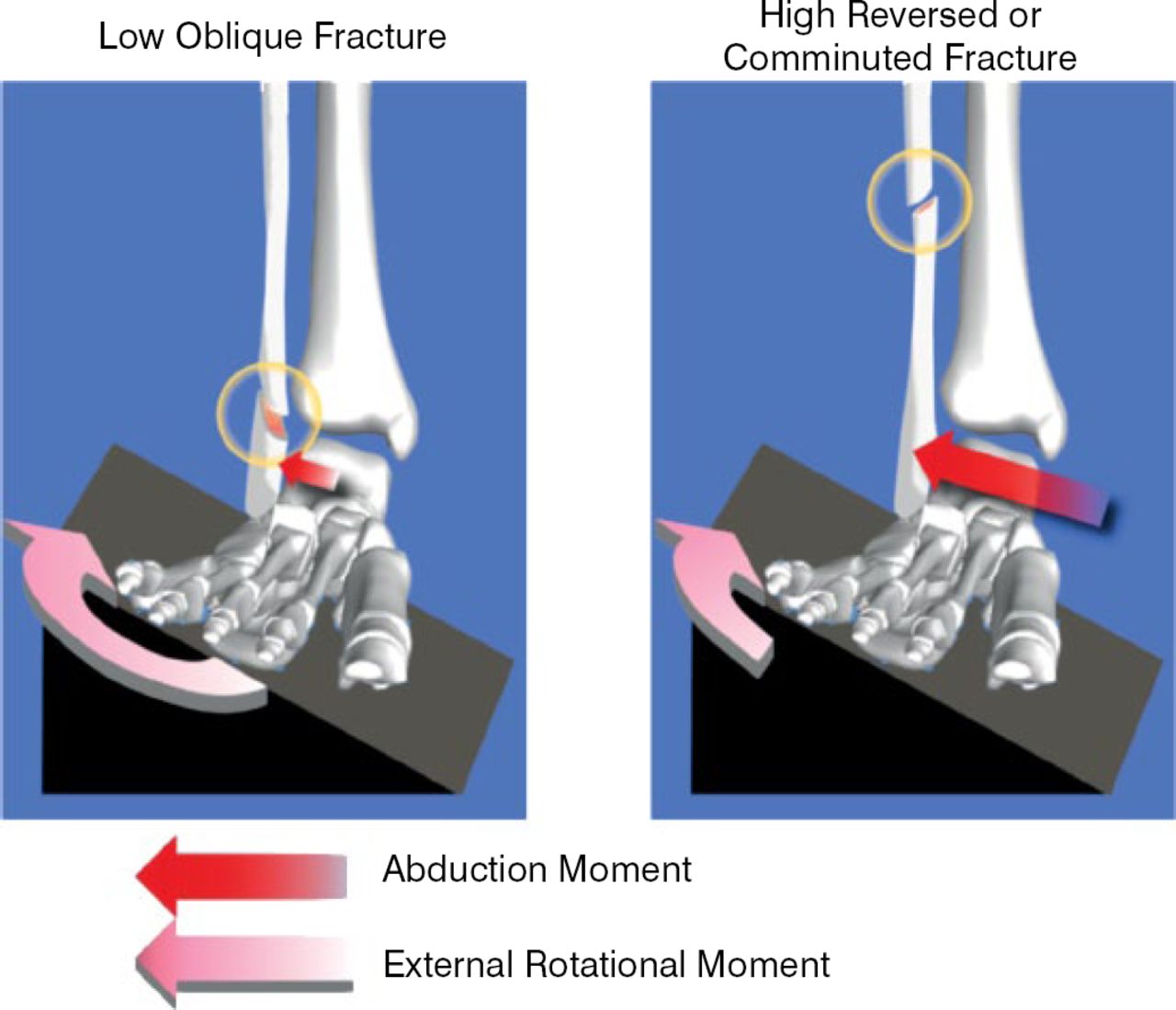
During phase I, 8 stage 4 S-E type fractures occurred and resulted in short spiral fractures of the fibula and the anterior inferior tibiofibular ligament (AITFL). All 8 specimens had both posterior and medial injury. In addition, there were posterior inferior tibiofibular ligament (PITFL) ruptures and avulsions, fractures of the medial and posterior malleolus, and rupture and avulsion of the deltoid. In phase II, increasing the external lateral force resulted in a high fibular fracture with a reversed fracture line and/or a comminuted high fibular fracture in 3 of the 8 specimens. Dr Haraguchi concluded by suggesting that classifying ankle injuries based on injury-producing loads instead of the Lauge-Hansen criteria could create a more logical classification of ankle fractures (Figure 1).

Classification Based on Injury-Producing Loads
Reproduced from Haraguchi N et al. A New Interpretation of the mechanism of ankle fracture. J Bone Joint Surg Am. 2009;91:821–829. With permission from The Journal of Bone and Joint Surgery, Inc.
Beat Hintermann, MD, University of Basel, Switzerland, spoke next of challenges involving the medial ankle ligament complex, which is crucial for ankle integrity and function. There is still, however, a paucity of knowledge regarding the anatomy and biomechanics of the ankle. He reviewed several methods of diagnosing deltoid ligament injuries, which range from stress testing to magnetic resonance imaging (MRI) and arthroscopy.
Prof Hintermann then moved on to discuss when and how acute deltoid injury should be treated. Although the evidence for treating deltoid injuries is sparse and the injury pattern can be difficult to predict, Prof Hintermann uses various imaging techniques and frequently will perform deltoid reconstruction. He believes that the positive outcomes include a stable, well-reduced ankle as well as the ability to avoid syndesmotic screw fixation. It is not clear whether surgical reconstruction can avoid medial ankle instability or secondary osteoarthritis.
Because there is very little published information regarding treatment for injuries to the spring ligament, Prof Hintermann shared some clinical pearls. He explained that the extent of ligament lesions is often greater than expected and is typically a distal lesion associated with a pronation deformity, and that the posterior tibial tendon is usually intact or may be elongated. The deformity can cause serious disability, and it is difficult to predict the extent and impact of the lesion. Because of his experiences with these types of injuries, he might recommend reconstruction, possible additional bony procedures, or arthrodesis.
According to some recently published and highly publicized data, patients with calcaneal fractures experienced no difference regardless of whether they underwent surgery or received nonoperative care [Griffin D et al. BMJ. 2014]. Ian Winson, MB, ChB, FRCS, Bristol, UK, highlighted the fact that although some randomized controlled trials have shown no simple difference between surgery and other treatments, it is not clear whether certain subgroups may benefit from a traditional surgery or what role a surgeon's expertise plays in eventual outcomes. Although open reduction internal fixation (ORIF) is still the gold standard in the United Kingdom, patients run the well-known risk of developing wound and other postsurgical complications. So is there another way to operate in a more safe and effective manner?
Mr Winson discussed some of the indications for percutaneous reduction with internal fixation (PRIF) techniques, such as tongue-type fractures and joint depression fractures. PRIF can restore the heel shape [Stulik J et al. J Bone Joint Surg Br. 2006] and allow for early range of motion because of better pain control. In addition, the timing of surgery is less critical and can help to eliminate wound problems. As an adjunct to ORIF, arthroscopy may be less time-consuming than X-rays or fluoroscopy in detecting incongruencies of intra-articular calcaneus fractures [Rammelt S et al. Foot Ankle Int. 2002].
Mr Winson concluded by emphasizing the benefits and drawbacks to percutaneous fixation techniques (Table 1).
Advantages and Disadvantages of Percutaneous Reduction Internal Fixation
Sergio Fernandez, MD, Clinica Santa Maria, Santiago, Chile, closed the panel with a discussion of whether screws or plates should be used to close midfoot (Lisfranc) lesions. He reviewed early evidence (from Myerson et al. in 1986) that approximately 65% of these lesions were caused by auto and motorcycle accidents. In 2014, that percentage had decreased to about one-third, with an increasing number of crush injuries, leading to a higher degree of soft tissue lesions [Yu X et al. Pak J Med Sci. 2014].
Evaluation of midfoot lesions should be made by the patient's history, the clinical situation, the time from volition to the hospital admission, and the characteristics of the soft tissue lesion. The next step is to obtain images, which can be static, dynamic, or comparative between weight bearing and non-weight bearing. Computerized tomography, however, will provide detailed images of subtle displacements and minor bone fragments. Dr. Fernandez also described various methods to classify skeletal and ligament lesions, highlighting a classification system offered by the Foot and Ankle Society of Argentina (Table 2).
Fracture Classification
Prof. Fernandez also reviewed the literature regarding which procedure is best for each of the evident fracture types. He recommended the use of screws for compression, fusion, and ligamentous fractures as well as for evident, simple, transarticular fixation. Bridge plating is a better choice for evident, complex comminuted fractures, and neutralization for evident, simple fractures.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.