

Summary
The newest findings in chronic obstructive pulmonary disease (COPD) were discussed by a panel that addressed recent clinical trials, an update of COPD exacerbations, recent developments in COPD comorbidities, and a report on the COPDGene study.
- Chronic Obstructive Pulmonary Disease
- Pulmonary Genomics
- Chronic Obstructive Pulmonary Disease
- Pulmonary Genomics
- Pulmonary & Respiratory Medicine
The newest findings in chronic obstructive pulmonary disease (COPD) were discussed by a panel that addressed recent clinical trials, an update of COPD exacerbations, recent developments in COPD comorbidities, and a report on the COPDGene study.
Barry J. Make, MD, National Jewish Health, Denver, Colorado, USA, delivered an update on clinical trials in COPD. In a study of 1142 patients, 250-mg once-daily azithromycin, added to usual treatment, reduced the risk of COPD exacerbations by 27% when compared with usual care [Albert RK et al. N Engl J Med. 2011]. The time to a first exacerbation was longer in the azithromycin group, and quality of life was improved. Inclusion criteria in this trial made it unlike other clinical trials in COPD—namely, a history of oxygen use and patients with Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage IV disease (very severe). Forty-eight percent of the participants were on triple therapy at entry. In a more recent study, patients with GOLD stage IV disease, smokers, and patients aged ≤ 65 years were less likely to respond to azithromycin [Han MK et al. Am J Respir Crit Care Med. 2014]. On the basis of these results, to reduce the risk of acute exacerbations in patients with COPD, Dr Make suggested considering azithromycin (off-label) for patients with GOLD stage II and III disease, nonsmokers, and older patients.
Step-down withdrawal of inhaled corticosteroids (ICSs) in patients with COPD with a history of exacerbation was not associated with an increase in the rate of moderate or severe COPD exacerbations compared with continuation of ICSs [Magnussen H et al. N Engl J Med. 2014]. The data suggest that starting an ICS on top of dual bronchodilators is not necessary if the goal is reduction of exacerbations, said Dr Make.
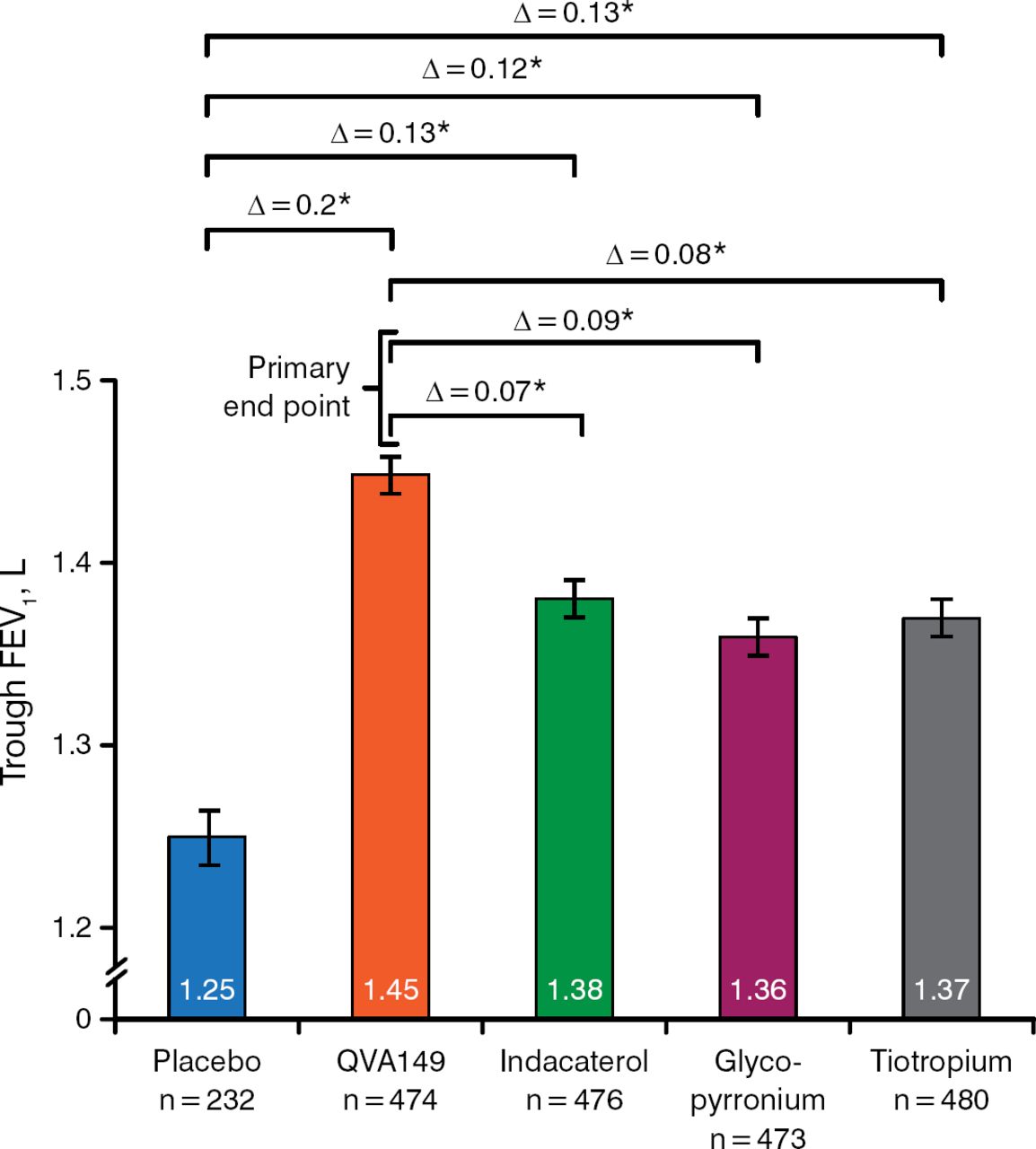
Dual bronchodilation improved trough forced expiratory volume at 1 second (FEV1) when compared with placebo and single-agent bronchodilation over 26 weeks (Figure 1) [Bateman ED et al. Eur Respir J. 2013] and improved shortness of breath as compared with placebo and single-agent bronchodilation over 6 weeks [Mahler DA et al. Eur Respir J. 2014].

Effect of Dual- vs Single-Agent Bronchodilation and Placebo on FEV1
FEV1, forced expiratory volume at 1 second.
*P < .001.
Adapted from Bateman ED et al. Dual bronchodilation with QVA149 vs single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42:1484–1494.
So-called comprehensive care management—consisting of education, an action plan, and proactive telephone case management—failed to decrease the rate of hospitalizations in patients with COPD and was associated with an increase in mortality compared with usual care [Fan VS et al. Ann Intern Med. 2012]. Dr Make questioned whether the intervention was actually comprehensive enough to be expected to have a positive impact.
High-dose N-acetylcysteine, 600 mg twice daily, reduced the frequency of COPD exacerbations as compared with placebo over 1-year follow-up, with no change in dyspnea, quality of life, or 6-minute walk distance [Tse HN et al. Chest. 2013].
Sanjay Sethi, MD, University at Buffalo, Buffalo, New York, USA, provided an update on studies of COPD exacerbations that may change practice relating to steroid use, antibiotics, and unreported exacerbations.
The REDUCE trial [Leuppi JD et al. JAMA. 2013] demonstrated that in patients with acute exacerbations of COPD, 5 days of systemic corticosteroid therapy was associated with comparable outcomes and a 1-day shorter length of stay when compared with 14 days of therapy, achieving a 65% reduction in steroid dose. The study suggests that a rethinking of high-dose prolonged steroid use to treat exacerbations is in order, said Dr Sethi.
Two studies showed that treating bacterial COPD exacerbations with corticosteroids may do harm, possibly by having an unfavorable effect on the microbiome. In outpatients with complicated bacterial acute exacerbation of COPD, clinical failure rates were higher with oral corticosteroid use in patients treated with antimicrobials [Wilson R et al. Eur Respir J. 2012]. Patients with neutrophilic bacterial-dominant exacerbations had higher rates of treatment failure with corticosteroid treatment when compared with placebo in a biomarker-directed randomized study [Bafadhel M et al. Am J Respir Crit Care Med. 2012].
Studies support the concept of antimicrobial treatment of acute exacerbations. Outpatients with mild to moderate acute exacerbations had a 73-day delay in their next exacerbation when treated with amoxicillin/clavulanate versus placebo [Llor C et al. Am J Respir Crit Care Med. 2012]. Clinical failure rates with moxifloxacin were noninferior to amoxicillin/clavulanate in a randomized controlled trial of patients with acute outpatient COPD exacerbations [Wilson R et al. Eur Respir J. 2012]. In this study, bacteriologic response at the end of therapy correlated with clinical cure at week 8 posttherapy.
In patients hospitalized with an acute exacerbation, 200 mg of doxycycline added to systemic corticosteroids for 7 days was no better than placebo on the outcomes of clinical cure or success at 30 days [Daniels JM et al. Am J Respir Crit Care Med. 2010]. The lesson from this study, said Dr Sethi, is that inadequate antibiotic therapy of an exacerbation can lead to frequent failures and relapses.
Patients with moderate to very severe COPD (GOLD stage II to IV) with ≥ 2 exacerbations (or ≥ 1 resulting in hospitalization) who are on optimal conventional management and are compliant with their treatment are candidates for macrolide treatment to reduce the frequency of exacerbations, while patients with unstable cardiovascular disease or hearing loss would not be candidates [Parameswaran GI, Sethi S. CMAJ. 2014].
A significant proportion of COPD exacerbations are unreported. An assessment of the performance of the Exacerbations of Chronic Pulmonary Disease Tool (EXACT)—a 14-question patient-reported outcome measure of COPD exacerbations—in 3 randomized controlled clinical trials found that 70% to 90% of EXACT-defined events were unreported [Leidy NK et al. Ann Am Thorac Soc. 2014]. In addition, only half of medically treated moderate events and 42% to 85% of medically treated severe events met the EXACT-defined threshold of an event, which raises uncertainty about how clinical events are defined, said Dr Sethi. Many of the unreported exacerbations are likely bacterial events, as bacterial colonization of the lower respiratory tract has been shown to increase daily symptoms in patients with COPD [Desai H et al. Ann Am Thorac Soc. 2014].
Nicola A. Hanania, MD, Baylor College of Medicine, Houston, Texas, USA, discussed recent developments in the comorbidities of COPD. More than half of patients with COPD report ≥ 4 comorbidities [Vanfleteren LE et al. Am J Respir Crit Care Med. 2013]. In the ECLIPSE study [Miller J et al. Respir Med. 2013], the most common COPD comorbidities reported were reflux, depression requiring treatment, and anxiety or panic attacks. Anxiety and depression in COPD patients led to an increase in symptoms, worse quality of life, and poorer functional status.
Systemic inflammation appears to be an important pathway that links COPD with its comorbidities, said Dr Hanania. Comorbidities are related to poor outcomes and increased mortality. A greater number of comorbidities in people with impaired lung function was associated with a shorter time to first hospitalization over 5-year follow-up [Mannino DM et al. Eur Respir J. 2008]. The number of comorbidities in COPD also correlates with mortality: 3 comorbidities double the risk of mortality, and ≥ 4 are associated with a >4-fold risk of mortality when compared with no comorbidities [Miller J et al. Respir Med. 2013]. Comorbidities also increase the cost of care in patients with COPD [Simon-Tuval T et al. Respir Res. 2011]. Anemia, which can occur in 15% of patients with COPD, correlates with systemic inflammation and is associated with more hospitalizations and duration of hospitalization [Chambellan A et al. Chest. 2005].
The prevalence of osteoporosis increases with COPD disease severity. When emphysema is present, the odds of osteopenia/osteoporosis increase >2-fold [Bon J et al. Am J Respir Crit Care Med. 2011]. Weight loss and muscle wasting are common in COPD. Increased breakdown of muscle proteins, a feature typical of cachexia, has been demonstrated in underweight patients with COPD [Agustí AG et al. Am J Respir Crit Care Med. 2002].
The effects of current treatments for COPD, except for pulmonary rehabilitation, on comorbidities have not been researched in prospective studies. The treatment of comorbidities in patients with COPD should be similar to treatment in patients without COPD, Dr Hanania said. Future studies of novel interventions for COPD should include patients with comorbidities.
Dr Make closed the session by offering lessons learned from some of the many analyses of the COPDGene study population. The goals of the study are to define genetic associations with COPD, phenotypes of COPD, pathophysiologic and mechanistic factors, the factors influencing disease progression, and the factors influencing response to therapy. It includes 10 059 patients with COPD (smokers, ex-smokers, and nonsmokers).
Of the first 2500 patients, 1061 have GOLD stages II to IV (290 with chronic bronchitis and 771 without). A study of the chronic bronchitic phenotype found that chronic bronchitis in COPD is associated with worse respiratory symptoms and almost twice the risk of exacerbations [Kim V et al. Chest. 2011]. Predictors of chronic bronchitis in COPD are histories of asthma, allergic rhinitis, and acute bronchitis; current smoking; a lower FEV1; Caucasian race; male sex; and airway thickening [Kim V et al. Respir Res. 2014]. Relative to controls without chronic bronchitis, genome-wide significant associations with chronic bronchitis were found on 4q22.1 (FAM13A) and 11p15.5 (EFCAB4A, CHID1, and AP2A2) and a locus associated with chronic bronchitis on 1q23.3 (RPL31P11 and ATF6) [Lee JH et al. Respir Res. 2014].
Quantitative computed tomography (CT) reveals that acute exacerbations of COPD are more frequent with worse emphysema and airway disease. Quantitative CT-defined airway disease was found to be more closely associated with worse quality of life on the St George's Respiratory Questionnaire than emphysema was [Martinez CH et al. Thorax. 2012]. The same study found that emphysema is more closely associated with the BODE index than airway disease is. Other lessons learned from chest CT scans are that interstitial lung abnormalities are common in smokers with COPD and that interstitial lung abnormalities is associated with a greater burden of disease [Doyle TJ et al. Am J Respir Crit Care Med. 2012].
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.