

Summary
The rates of contralateral prophylactic mastectomy are increasing in the United States, at the expense of unilateral mastectomy and breast-conserving surgery. Reasons include an overestimation of the risk of developing contralateral breast cancer, anxiety, an increase in the use of genetic testing, and a desire for better breast symmetry.
- bilateral mastectomy
- unilateral breast cancer
- clinical implication
- risk perception
- patient preference
Rates of contralateral prophylactic mastectomy (CPM) or bilateral mastectomy to treat unilateral breast cancer have been increasing as a proportion of all mastectomies. Ismail Jatoi, MD, PhD, University of Texas Health Science Center, San Antonio, Texas, USA, discussed the clinical implications of CPM.
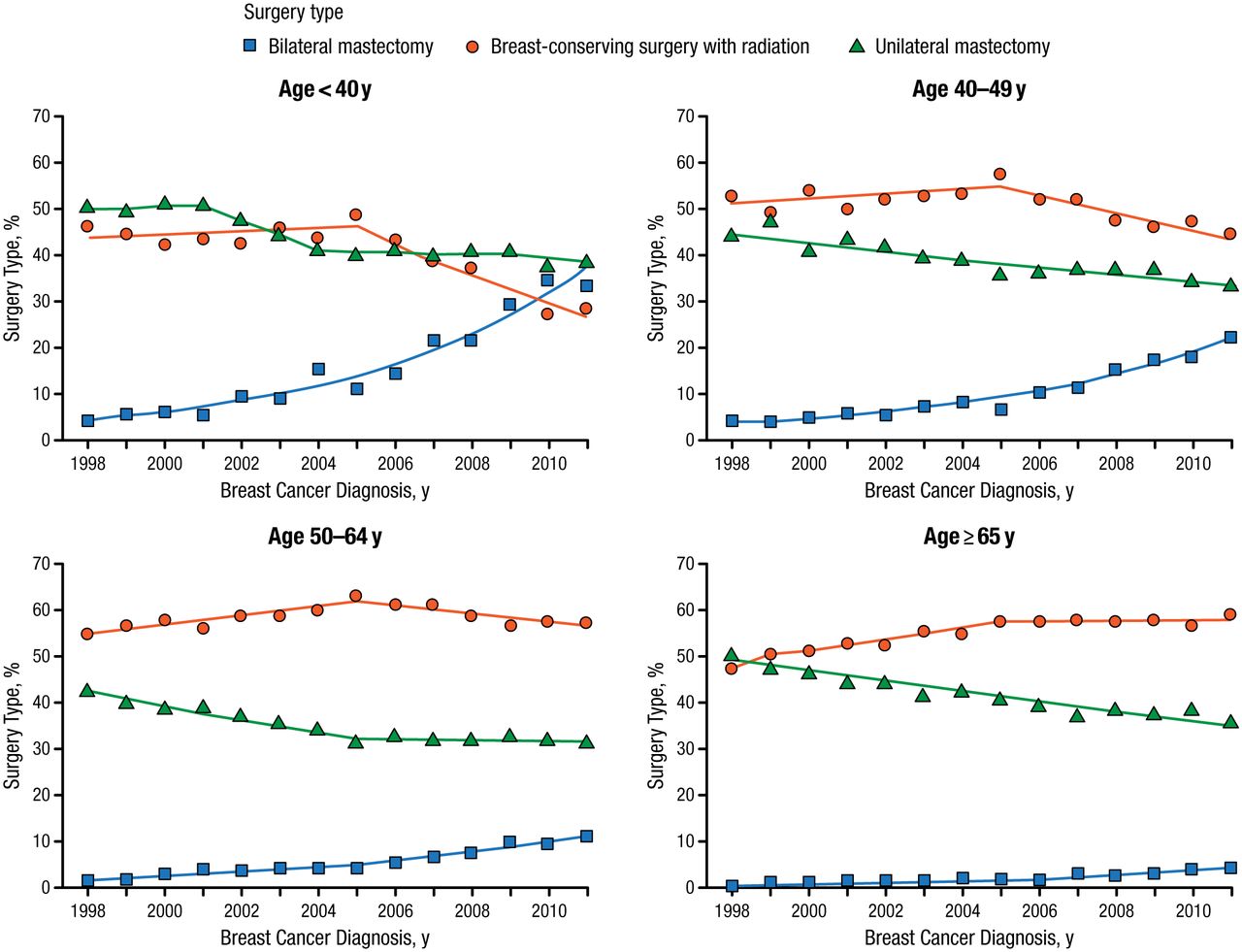
The rates of CPM are increasing in the United States. Data from 1998 to 2011 show a striking decrease in unilateral mastectomy, a stabilization of breast-conserving surgery, and a concomitant increase in bilateral mastectomy (Figure 1) [Kurian AW et al. JAMA. 2014]. These changes have occurred despite a decline in the annual hazard rates for contralateral breast cancer (CBC) over time [Nichols HB et al. J Clin Oncol. 2011] and a lack of evidence to suggest that CPM is associated with a survival benefit, noted Dr Jatoi.

Trends in Breast Cancer Surgery Type, by Patient Age at Diagnosis
Adapted from Kurian AW et al. Use of and mortality after bilateral mastectomy compared with other surgical treatments for breast cancer in California, 1998-2011. JAMA. 2014;312:902-914. Copyright © (2014) American Medical Association. All rights reserved.
The underlying reason for these trends is not fully understood, but a potential explanation is that women may overestimate their risk of developing CBC. Several other potential factors to account for increased rates of CPM may be younger age, a preference for better symmetry with bilateral mastectomy and reconstruction vs unilateral mastectomy and reconstruction, an increase in the use of genetic testing, and wider use of preoperative breast magnetic resonance imaging [Hawley ST et al. JAMA Surg. 2014]. In addition, observational studies that demonstrate reductions in breast cancer–specific and all-cause mortality compared with unilateral surgical treatment alone may influence patients’ decisions. These reductions in mortality, however, may reflect a confounding bias, such as selection of a healthier cohort for CPM, he said.
To explore this possibility, Dr Jatoi’s group examined the association between CPM and noncancer mortality in 449 178 adult women diagnosed with unilateral primary American Joint Committee on Cancer (AJCC) stage I to III ductal or lobular breast cancer, using the 1998–2010 Surveillance, Epidemiology, and End Results data set [Jatoi I, Parsons HM. Breast Cancer Res Treat. 2014]. Of these women, 5.8% (n = 25 961) underwent CPM as their first course of treatment. Multivariate logistic regression—adjusting for age, race, AJCC stage, estrogen receptor status, progesterone receptor status, and histologic grade of the tumor—showed that among all patients receiving CPM as a first course of treatment, CPM was associated with lower breast cancer–specific (HR 0.84; 95% CI, 0.79 to 0.89), all-cause (HR 0.83; 95% CI, 0.80 to 0.88), and noncancer (HR 0.71, 95% CI, 0.64 to 0.80) 5-year hazard of death. The even stronger association between CPM and lower noncancer mortality compared with breast cancer–specific and all-cause mortality is evidence that selection bias is partially attributable for reported associations between CPM and reductions in mortality.
Ann H. Partridge, MD, MPH, Dana-Farber Cancer Institute, Boston, Massachusetts, USA, spoke about patient preferences and risk perceptions about CPM. In a cross-sectional survey, women reported high overall satisfaction with their decision to have CPM [Rosenberg SM et al. Ann Intern Med. 2013]. Of 123 women with unilateral breast cancer who were ≤ 40 years at diagnosis and had undergone bilateral mastectomy (only 25% of whom were BRCA1/BRCA2 mutation carriers), 90% would definitely have chosen CPM if they had to make the decision again, and 97% believed that they knew the risks and benefits of each treatment option.
Decisions are potentially being made without adequate information and psychosocial support. Physicians were the most important sources of information in the decision to undergo CPM; 80% of women reported speaking with their physicians to at least some extent about the reasons for having CPM [Rosenberg SM et al. Ann Intern Med. 2013]. Few women reported advice from family or friends or abnormal screening tests as important reasons for choosing CPM.
Further, women are making decisions about CPM based on inaccurate risk perceptions and understanding. Women who were not at increased genetic risk (noncarriers of BRCA1/BRCA2 mutation) overestimated their chance of developing a CBC, with noncarriers estimating that a median of 10 of 100 women would develop a CBC without CPM within 5 years [Rosenberg SM et al. Ann Intern Med. 2013], which exceeds the actual risk of approximately 2% to 4% over 5 years.
Anxiety and fear of recurrence are stoking inaccurate risk perceptions among those with breast cancer. Most women ranked desire to improve survival and a desire to prevent metastatic disease as extremely or very important reasons for choosing CPM, even though most understood that having a bilateral mastectomy would not lead to an extension of survival [Rosenberg SM et al. Ann Intern Med. 2013]. In another survey of 1447 women with breast cancer, 68.9% of women who underwent CPM had no major genetic or familial risks for CBC [Hawley ST et al. JAMA Surg. 2014].
Physicians must offer patient-centered care, ensuring that risks and benefits are effectively communicated in a supportive environment, with the goal of shared decision making, said Dr Partridge.
Andrea Pusic, MD, Memorial Sloan-Kettering Cancer Center, New York, New York, USA, discussed the implications of CPM for reconstruction, noting that women with breast cancer increasingly seek information on reconstructive options and outcomes. Options for reconstruction are flap reconstruction and tissue expansion with implant, both with nipple reconstruction. Flap reconstruction uses autologous tissue, usually from the abdomen, that is relocated to form a new breast mound. In tissue expansion, a temporary inflatable breast implant put in place for 3 to 6 months stretches the skin and pectoralis muscle to accommodate a permanent implant.
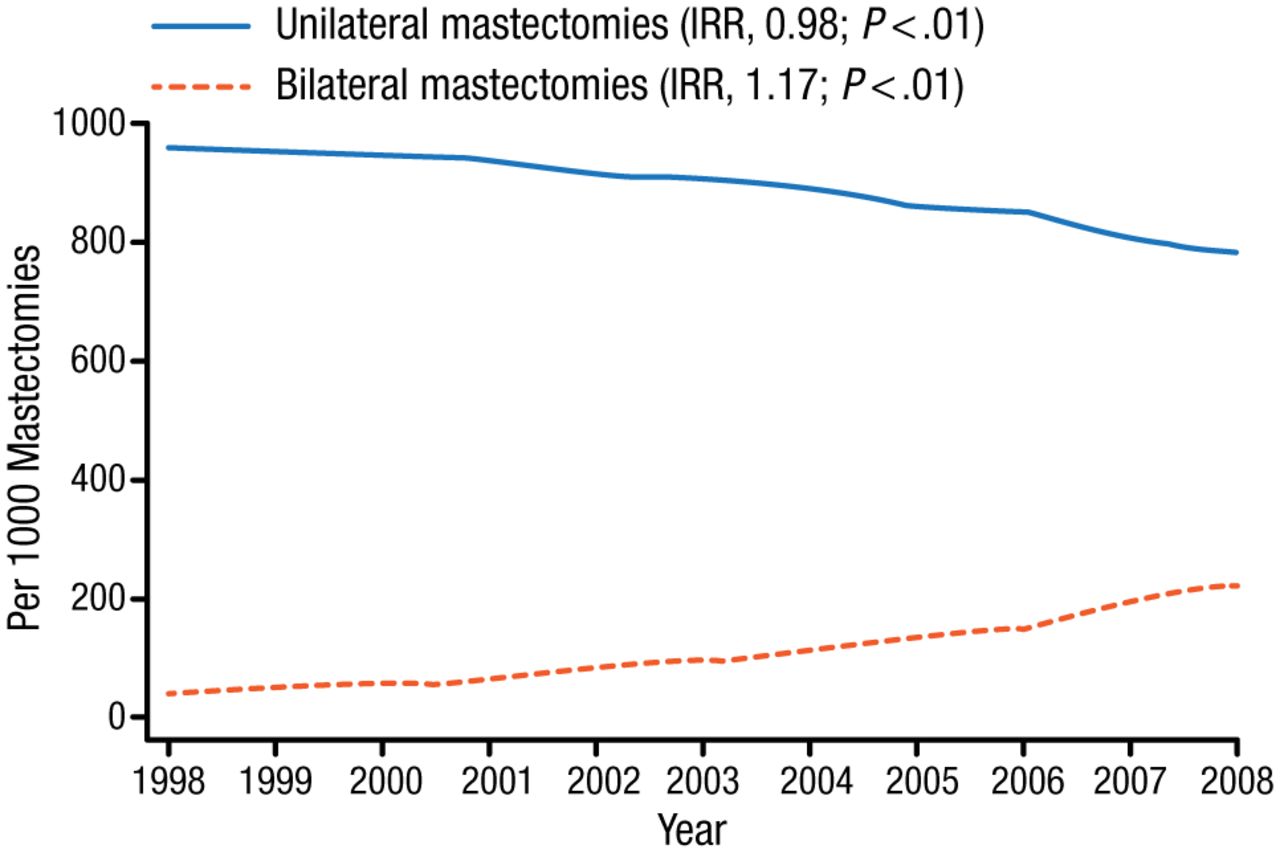
The popularity of implant reconstruction is increasing, more than doubling between 1998 and 2008, and has increased for bilateral mastectomies by 17% per year (Figure 2) [Albornoz CR et al. Plast Reconstr Surg. 2013].

Unilateral and Bilateral Mastectomy Rates, US, 1998 to 2008
IRR, incidence rate ratio.
Reprinted from Albornoz C et al. A paradigm shift in U.S. breast reconstruction: increasing implant rates. Plast Reconstr Surg. 2013;131:15-23.
The changing mastectomy pattern (increasing use of bilateral mastectomies) is one factor that underlies a shift away from use of autologous tissue to implant-based reconstruction [Cemal Y et al. Plast Reconstr Surg. 2013]. Responses to a patient questionnaire showed that more than one third of mastectomy patients chose bilateral mastectomy because they wanted breast symmetry [Han E et al. Am J Surg. 2011].
Unilateral implant reconstruction can be disappointing in the long term, said Dr Pusic, and patients must be made aware of expected outcomes. A new way of measuring patient satisfaction/quality of life with breast reconstruction is a questionnaire called the Breast-Q. Among 294 women who used the instrument to measure satisfaction with breast reconstruction, the mean satisfaction score was higher among the 112 who underwent bilateral reconstruction compared with the 182 who had unilateral reconstruction at a mean of 4.5 years (P = .001), but quality-of-life domains did not differ [Koslow S et al. Ann Surg Oncol. 2013].
Postmastectomy reconstruction with a direct implant offers a 1-step approach to reconstruct the breast mound in select patients. Direct implant placement forgoing tissue expansion is an appealing option to women, she said, and is best suited for patients with preserved breast skin after mastectomy.
- © 2014 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.