

Summary
“Wake-up” strokes occur when an individual wakes up with neurological deficits from a stroke. The most frequent time of onset for all subgroups of ischemic stroke is between 6 am and 12 pm [Marsh EE et al. Arch Neurol 1990]. Retrospective studies have shown that wake-up stroke is common, with a prevalence of approximately 14% to 28%. Although tissue plasminogen activator (tPA) significantly improves outcomes [Hacke W et al. N Engl J Med 2008], patients with wake-up stroke are often not eligible for this therapy because the medication must be given within 4.5 hours of when the patient was last known to be normal. This article discusses the epidemiology, clinical features, and available data for the effectiveness of thrombolytic treatment in patients with wake-up stroke.
- Thrombotic Disorders
- Ischemia
- Neurology
- Thrombotic Disorders
- Ischemia
“Wake-up” strokes occur when an individual wakes up with neurological deficits from a stroke. The most frequent time of onset for all subgroups of ischemic stroke is between 6 am and 12 pm [Marsh EE et al. Arch Neurol 1990]. Retrospective studies have shown that wake-up stroke is common, with a prevalence of approximately 14% to 28%. Although tissue plasminogen activator (tPA) significantly improves outcomes [Hacke W et al. N Engl J Med 2008], patients with wake-up stroke are often not eligible for this therapy because the medication must be given within 4.5 hours of when the patient was last known to be normal. Epidemiology, clinical features, and available data for the effectiveness of thrombolytic treatment in patients with wake-up stroke were described in this session.
Jason Mackey, MD, Indiana University, Indianapolis, Indiana, USA, addressed the epidemiology of wake-up strokes. The Greater Cincinnati/Northern Kentucky Stroke Study [GCNKSS] was a large population-based investigation that compared patients with wake-up stroke with those who were awake at the time of symptom onset [Mackey J et al. Neurology 2011]. Of 1854 patients presenting to an emergency department with ischemic stroke, 14.3% had a wake-up stroke (adjusted wake-up stroke event rate, 26.0/100,000; 95% CI, 22.9 to 29.1). Extrapolated to the nation as a whole, the authors estimated that 58,000 patients presented to an emergency department with a wake-up stroke in 2005. The authors also estimated that at ≥35.9% of the wake-up stroke patients would have been eligible for thrombolysis if arrival time were not a factor.
Whether there are differences between wake-up strokes and other strokes is unclear. In GCNKSS, wake-up stroke patients were more likely to be older. Other studies have suggested that obesity [Jiménez-Conde J et al. J Neurol 2007] and smoking [Nadeau JO et al. Can J Neurol Sci 2005] might increase the risk for wake-up stroke.
It is also unclear whether there is a difference in severity between wake-up and awake stroke. Some studies have shown wake-up stroke to be more severe [Huisa BN et al. J Stroke Cerebrovasc Dis 2010; Jiménez-Conde J et al. J Neurol 2007; Kim BJ et al. Stroke 2011; Mackey J et al. Neurology 2011], but at least one study has shown awake stroke to be more severe [Fink JN et al. Stroke 2002] and another found no difference [Serena J et al. Cerebrovasc Dis 2003]. Outcomes have also been mixed. There was no significant difference in 90-day mortality (approximately 16% in both groups) in GCNKSS, but 1 recent small study showed that wake-up stroke patients fared better, although this benefit was not statistically significant [Huisa BN et al. J Stroke Cerebrovasc Dis 2010]. Other studies have shown that wake-up stroke patients do worse, with patients being less likely to return home [Nadeau JO et al. Can J Neurol Sci 2005] and having worse functional outcomes at 3 months [Jiménez-Conde J et al. J Neurol 2007].
Victor C. Urrutia, MD, The Johns Hopkins Hospital Stroke Center, Baltimore, Maryland, USA, discussed the circadian variation in stroke, and several studies that assessed early ischemic changes detected on computed tomography (CT) and magnetic resonance imaging (MRI) in patients with wake-up and awake stroke.
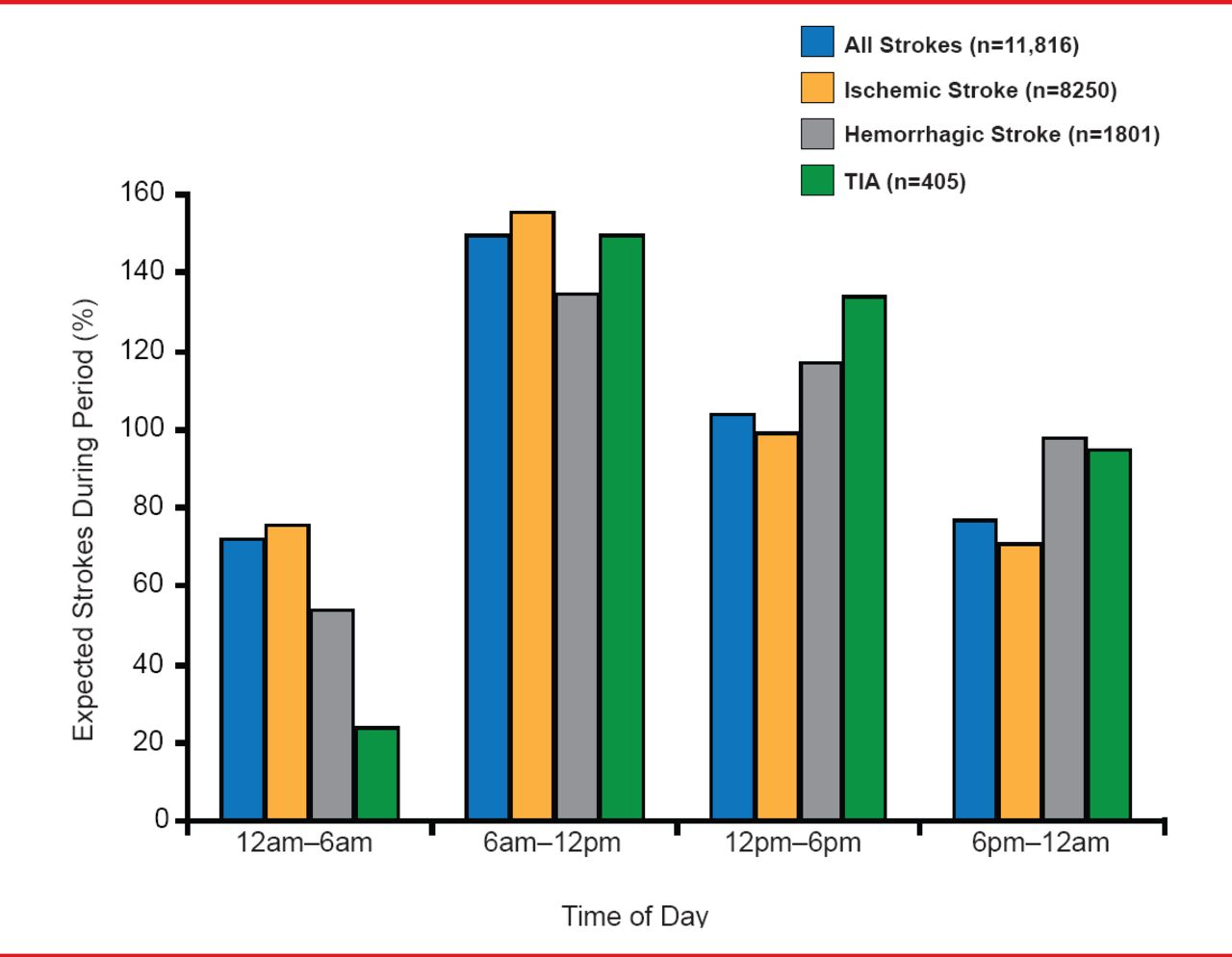
A circadian variation for stroke occurrence appears well established with relative risk for early morning stroke being 49% compared with the number expected if strokes were distributed evenly throughout the day (95% CI, 44 to 55; Figure 1) [Elliott WJ. Stroke 1998]. Potential causes for the circadian rhythm include coagulability [Jafri SM et al. Am J Cardiol 1992]; fibrinolysis [Jovicic A, Mandic S. Thrombosis Res 1991]; platelet aggregation [Andrews NP et al. J Am Coll Cardiol 1996]; elevated epinephrine, norepinephrine, and cortisol levels; and higher blood pressure in the morning [Panza JA et al. N Engl J Med 1991; Stergiou GS et al. Stroke 2002].
In a recent study that assessed ischemic changes detected on CT, Huisa and colleagues [J Stroke Cerebrovasc Dis 2010] found no difference in Alberta Stroke Program Early CT Score (ASPECTS) between patients whom they named “AWOKE” (patients likely to have wake-up strokes defined as having a last seen normal time >4 hours but <15 hours, and presenting to the Emergency department between 4 am and 10 am) and a control group of patients with awake stroke of known onset time.
In the study, 89.3% of patients in the wake-up stroke group versus 95.6% of control group patients had an ASPECTS of 8 to 10 (p=0.353). Although more patients in the AWOKE group had a modified Rankin Scale (mRS) score of 0 to 1 at 90 days compared with control, the difference was not significant (73% vs 45%; p=0.079) [Huisa BN et al. J Stroke Cerebrovasc Dis 2010]. Diffusion-weighted- (DWI) and perfusion-weighted imaging (PWI) lesion volumes as well as DWI-PWI mismatch were similar between the 2 groups [Fink JN et al. Stroke 2002]. Additionally, it has recently been shown that fluid-attenuated inversion recovery (FLAIR) data can be used to identify patients with time from symptom onset ≤4.5 hours with high specificity; however, sensitivity is low [Cheng B et al. J Cereb Blood Flow Metab 2013; Thomalla G et al. Lancet Neurol 2011].

Circadian Patterns of Onset of Stroke Symptoms
TIA=transient ischemic attack.
Reproduced from Elliott WJ et al. Circadian Variation in the Timing of Stroke Onset: A Meta-analysis. Stroke 1998;29(5):992–996. With permission from Lipincott Williams and Wilkins.
According to Dr. Urrutia, the circadian data and the FLAIR, CT, and MRI studies support the hypothesis that wake-up stokes have their onset upon awakening, suggesting that these patients could benefit from tPA therapy if they arrive to the hospital within the 4.5-hour time window. Studies are needed to confirm this hypothesis.
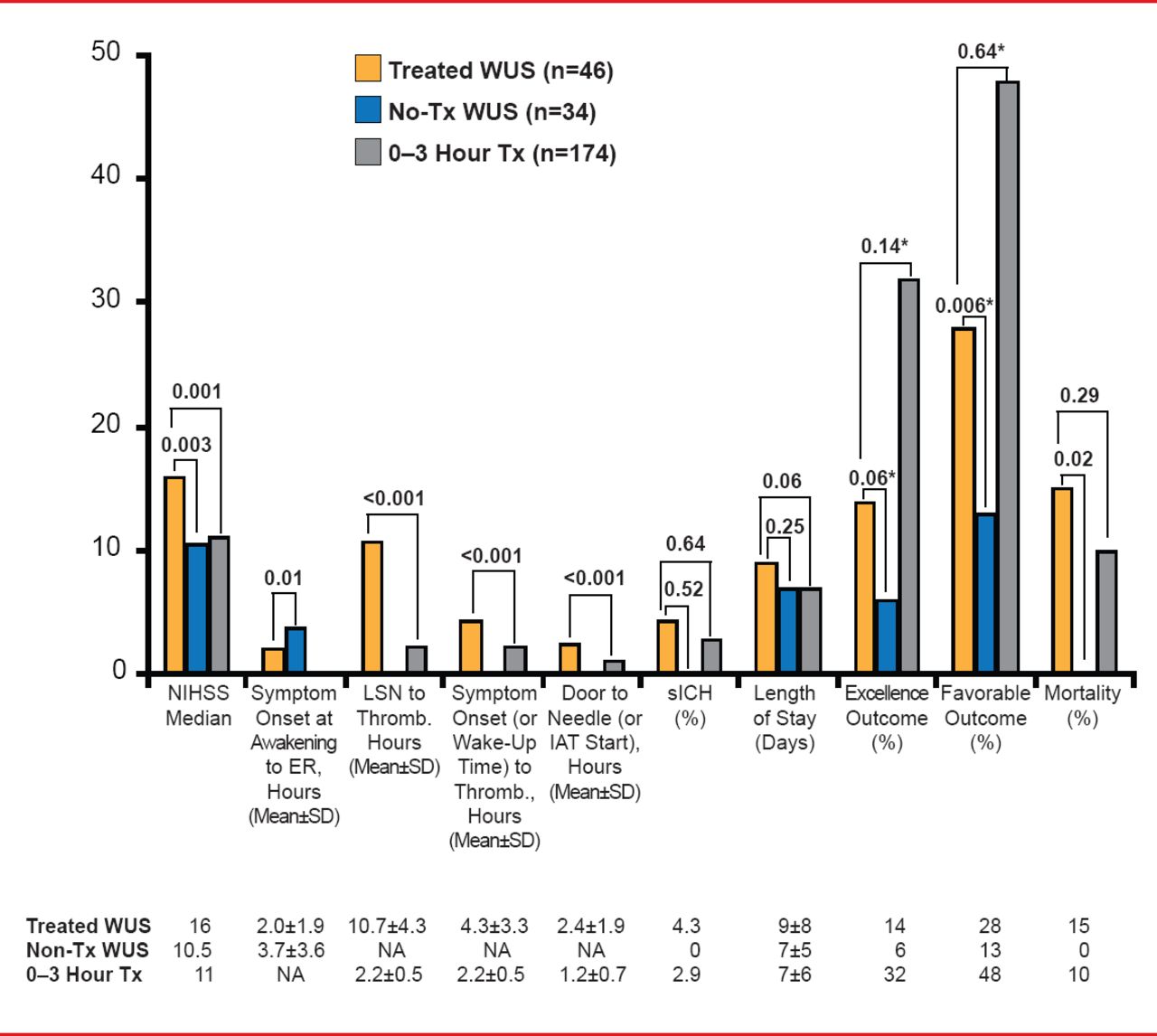
Dulka Manawadu, MD, King's College Hospital, London, United Kingdom, believes it is feasible and safe to thrombolyze wake-up stroke patients with clinical and imaging features comparable to patients with a known time of stroke onset. In a compassionate use with consent study, wake-up stroke patients who received thrombolysis had higher rates of excellent (mRS score 0 to 1; 14% vs 6%; p=0.06) and favorable (mRS score 0 to 2; 28% vs 13%; p=0.006) outcomes but higher mortality (15% vs 0%) compared with nontreated wake-up stroke patients (Figure 2) [Barreto AD et al. Stroke 2009].

Interventional Wake-Up Stroke Studies
Controlled for baseline NIHSS.
ER=emergency room; IAT=intra-arterial therapy; LSN=last-seen-normal; NIHSS=National Institute of Health Stroke Scale; sICH=symptomatic intracerebral hemorrhage; Thromb=thrombolysis; Tx=thrombolytics; WUS=wake-up stroke.
Reproduced from Barreto AD et al. Thrombolytic Therapy for Patients Who Wake-Up With Stroke. Stroke 2009;40(3):827–832. With permission from Lipincott Williams and Wilkins.
Dr. Manawadu and colleagues conducted a similar study that compared baseline characteristics and clinical outcomes at 90 days between thrombolyzed wake-up stroke patients (n=68), nonthrombolyzed wake-up stroke patients (n=54) [Manawadu D et al. Stroke 2013], and patients who received thrombolysis at 0 to 4.5 hours of stroke onset (n=326). Median changes in National Institute of Health Stroke Scale (NIHSS) at 24 hours, 90-day mRS scores, and 90-day mortality were similar between the 3 groups. Although symptomatic intracerebral hemorrhage (ICH) was not different, ICH was significantly lower (p=0.004) in nonthrombolyzed (3.7%) versus thrombolyzed wake-up stroke patients (22%), and the non-wake-up thrombolyzed group (20%). The authors concluded that thrombolysis in wake-up stoke patients is possible and may improve outcomes in these patients.
Andrew D. Barreto, MD, University of Texas Health Science Center at Houston, Houston, Texas, USA, reported on 10 mostly prospective, ongoing studies of wake-up stroke and thrombolytics (thrombolysis for wake-up stroke). The studies have variable patient selection and neuroimaging protocols, as well as different inclusion criteria. Dr. Barreto feels that reproducibility in the community setting will prove challenging and investigators should consider collaboration to combine efforts. Despite the pro-thrombolysis leanings of the presenters for wake-up stroke patients, he pointed out that it is too early to give the go-ahead for the use of tPA in this group of patients.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.