

Summary
Nonemergency percutaneous coronary intervention (PCI) performed at hospitals without on-site cardiac surgery capability, but with sufficient procedural volume was as safe and effective as PCI performed at hospitals with cardiac surgery services. This article presents results from a Randomized Trial to Compare Percutaneous Coronary Intervention Between Massachusetts Hospitals With Cardiac Surgery-On-Site and Community Hospitals Without Cardiac Surgery-On-Site [MASS COM; Jacobs AK et al. N Engl J Med 2013] which compared the outcomes of nonemergency PCI at 10 hospitals in Massachusetts without on-site cardiac surgery services and 7 hospitals with on-site cardiac surgery services.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology
Nonemergency percutaneous coronary intervention (PCI) performed at hospitals without on-site cardiac surgery capability, but with sufficient procedural volume was as safe and effective as PCI performed at hospitals with cardiac surgery services.
Alice Jacobs, MD, Boston University, Boston, Massachusetts, USA, presented results from a Randomized Trial to Compare Percutaneous Coronary Intervention Between Massachusetts Hospitals With Cardiac Surgery-On-Site and Community Hospitals Without Cardiac Surgery-On-Site [MASS COM; Jacobs AK et al. N Engl J Med 2013] which compares the outcomes of nonemergency PCI at 10 hospitals in Massachusetts without on-site cardiac surgery services and 7 hospitals with on-site cardiac surgery services.
Since emergency coronary artery bypass graft surgery is rare following PCI, it raises the question of whether on-site cardiac surgery is still necessary for the performance of safe and effective PCI, said Dr. Jacobs. The need for patients with ST-elevation myocardial infarction to have timely access to PCI has justified expansion of emergency (primary) PCI to hospitals without on-site cardiac surgery. Further expansion to the nonemergency setting has been controversial because of an uncertain risk:benefit ratio.
In MASS COM, short-term safety and 12-month outcomes were assessed in 3691 patients who were randomly assigned in a 3:1 ratio to undergo PCI at hospitals without on-site cardiac surgery (n=2774) or at hospitals with surgical back-up (n=917). The primary safety endpoint was death, myocardial infarction (MI), stroke, or repeat revascularization at 30 days while efficacy for the same endpoint was assessed at 12 months. The study was designed to test for noninferiority (using noninferiority margins of 1.5 for safety and 1.3 for effectiveness) on an intent-to-treat basis. A random sample of 376 of enrolled subjects was selected to monitor clinical practice patterns of the hospitals.
Hospital and operator requirements for participation included a minimum of 75 PCI procedures performed annually. Hospitals without on-site cardiac surgery were required to have a signed collaboration agreement with an on-site surgery hospital for backup and to perform a minimum of 300 diagnostic procedures in each of the previous 2 years and a minimum of 36 primary PCI procedures per year.
Baseline characteristics were similar between the 2 groups, but more patients randomized to hospitals without on-site surgery had a prior history of MI compared with those randomized to hospitals with on-site surgery (24.1% vs 20.2%; p=0.015).
There were no significant differences between the 2 treatment groups with respect to procedural success rates, completeness of revascularization, or the proportion of lesions that met indication criteria for PCI. However, patients treated at hospitals without on-site surgery received drug-eluting stents less often than those treated at hospitals with on-site surgery (63.7% vs 69.3%; p<0.001).
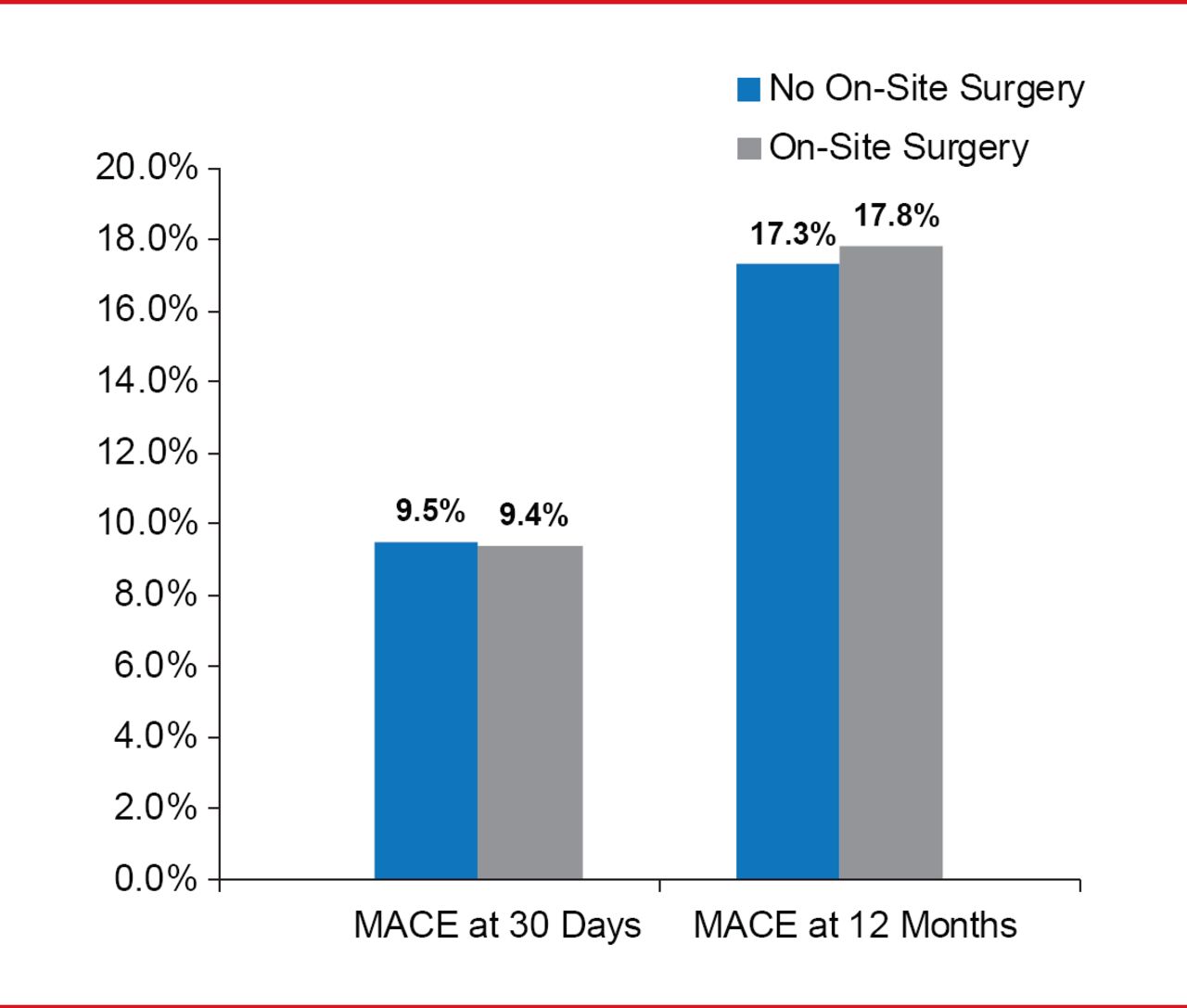
The 30-day primary safety endpoint—a composite of death, MI, stroke, or repeat revascularization—occurred in 9.5% of patients treated at sites without on-site cardiac surgery compared with 9.4% in those treated at sites with surgical services (p<0.001 for noninferiority; Figure 1).
The primary efficacy endpoint of death, MI, stroke, or repeat revascularization at 12 months did not differ across groups—17.3% for sites without on-site surgery compared with 17.8% for sites with surgical services available (p<0.001 for noninferiority; Figure 1). Seven patients (0.25%) randomized to sites without surgery required transfer to a hospital for emergency surgery of whom none died.

Primary Safety and Efficacy Endpoints
MACE=major adverse cardiac events
There was also no difference between groups in occurrence of secondary endpoints of target lesion revascularization, target vessel revascularization, and stent thrombosis at either 30 days or 12 months, and major vascular complications at 30 days (Table 1).
Occurrence of Secondary Endpoints
PCI performed at hospitals in Massachusetts without cardiac surgery on site was noninferior to PCI performed with cardiac surgery on site with respect to the 30-day safety and 12-month effectiveness endpoints, Dr. Jacobs concluded. These data suggest that PCI can be safely performed at hospitals without surgery on site and could be an acceptable option for patients if the facility and individual operators have the requisite amount of experience.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.