

Summary
Structured screening for heart failure (HF) using measurement of B-type natriuretic peptide (BNP) followed by targeted collaborative care was effective at preventing left ventricular dysfunction and HF in a community setting. The use of biomarkers related to ventricular damage or dysfunction may improve the ability to identify individuals at risk and ultimately prevent downstream complications. Because it reflects established cardiovascular (CV) insult rather than CV risk, BNP might help identify high risk patients and help focus care where it is needed most, according to the rationale for the St. Vincent's Screening to Prevent Heart Failure study [STOP-HF; NCT00921960].
- Heart Failure
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Heart Failure
- Cardiology Clinical Trials
Structured screening for heart failure (HF) using measurement of B-type natriuretic peptide (BNP) followed by targeted collaborative care was effective at preventing left ventricular dysfunction (LVD) and HF in a community setting.
Using clinical criteria alone to identify patients who may be at risk for HF and instituting preventive therapy has been shown to be of relatively limited value. The use of biomarkers related to ventricular damage or dysfunction may improve the ability to identify individuals at risk and ultimately prevent downstream complications. Because it reflects established cardiovascular (CV) insult rather than CV risk, BNP might help identify high risk patients and help focus care where it is needed most, said Kenneth McDonald, MD, Heart Failure Unit, St. Vincent's University Hospital, Dublin, Ireland, in providing the rationale for the St. Vincent's Screening to Prevent Heart Failure study [STOP-HF; NCT00921960].
STOP-HF was conducted in 39 collaborating primary-care practices referring into one CV center in Dublin, and enrolled asymptomatic patients aged >40 years with at least one risk factor for HF (such as hypertension, hyperlipidemia, diabetes, vascular disease, arrhythmia, and obesity).
Of the 1374 patients randomized, those in the intervention group (n=697) were screened annually with BNP measurement and underwent echocardiography and other tests in consultation with a cardiologist if the BNP was >50 pg/mL, while those in the control group (n=677) received standard care from their primary physicians (Table 1). The primary endpoint was the prevalence and severity of LVD (defined as left ventricular ejection fraction <50% [systolic] or E/e prime >15 [diastolic] and measured by Doppler echocardiography). The secondary endpoint was incidence of major adverse cardiac events (MACE), defined as HF, arrhythmia, myocardial infarction, unstable angina, cerebrovascular event, transient ischemic attack, pulmonary embolism, or peripheral thrombosis.
STOP-HF Intervention and Routine Care
About one fourth of the patients in each group had 3 or more risk factors for HF, with hypertension the most prevalent, present in ∼60% in each group. The mean BNP was 47 pg/mL and mean systolic blood pressure was 146 mm Hg.
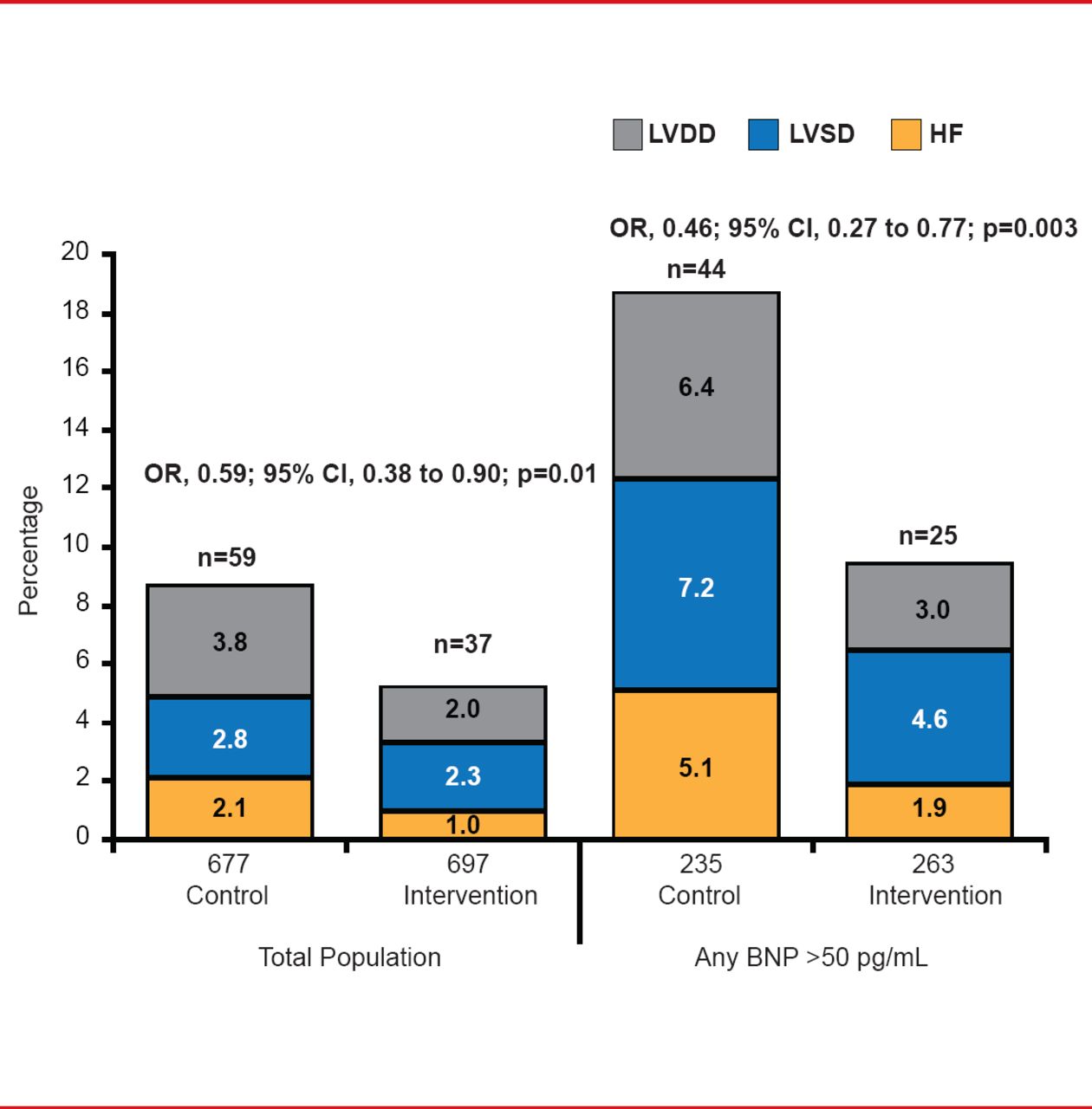
After a mean follow-up of 4.2 years, the odds of achieving the primary endpoint were 41% lower in the intervention group compared with the control group (5.3% vs 8.7%; OR, 0.59; 95% CI, 0.38 to 0.90; p=0.01; Figure 1). The reduction in risk in the intervention group was driven primarily by a 54% reduction in the rate of primary endpoint episodes in patients with any BNP level >50 pg/mL (9.5% in the intervention group vs 18.7% in the control group; 0.46; 95% CI, 0.27 to 0.77; p=0.003; Figure 1).

Components of Primary Endpoint
BNP=B-type natriuretic peptide; HF=heart failure; LVDD=left ventricular diastolic dysfunction; LVSD=left ventricular systolic dysfunction.
Reproduced with permission from K McDonald, MD.
The secondary endpoint of MACE was reduced by 33% in the intervention group relative to controls (OR, 0.66; 95% CI, 0.46 to 0.98; p=0.04). In the subgroup of patients with BNP >50 pg/mL, MACE events occurred in 10.5% of patients in the control group compared with 7.3% in the intervention group, corresponding to a 46% reduction in the odds ratio with intervention (OR, 0.54; p=0.001).
The major therapeutic change in patients assigned to the intervention was the greater use of inhibitors of the renin-angiotensin-aldosterone system (p=0.02). There was a trend toward a lower level of low-density lipoprotein cholesterol in patients assigned to intervention (p=0.06), despite similar use of statin therapy, implying that compliance and adherence may have been improved with the intervention. The increase in BNP level over time was attenuated in the patients randomized to the intervention.
These results suggest that BNP may be a useful adjunctive tool to identify patients at risk for clinical HF or LVD but additional data is needed before this strategy is applied in routine clinical practice.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.