

Summary
In patients with paroxysmal atrial fibrillation (PAF), disease can be eliminated by targeting ablation to its primary sustaining mechanism alone without the need to ablate triggers. This is the conclusion of the Precise Rotor Elimination without Concomitant pulmonary vein Isolation for the Successful Elimination of Paroxysmal Atrial Fibrillation study [PRECISE-PAF; NCT01248156] presented in a late-breaking clinical trial session.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Arrhythmias
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Arrhythmias
In patients with paroxysmal atrial fibrillation (PAF), disease can be eliminated by targeting ablation to its primary sustaining mechanism alone without the need to ablate triggers. This is the conclusion of the Precise Rotor Elimination without Concomitant pulmonary vein Isolation for the Successful Elimination of Paroxysmal Atrial Fibrillation study [PRECISE-PAF; NCT01248156] presented in a late-breaking clinical trial session.
The study results also confirm recently published evidence that the primary sustaining mechanisms of PAF is by stable rotors and focal sources revealed by Focal Impulse and Rotor Map (FIRM) in patient-specific bi-atrial locations [Narayan SM et al. J Am Coll Cardiol 2012], and offers data that elimination of rotors or focal sources either directly by FIRM-guided ablation, or coincidentally when anatomical ablation passes through them, may explain the success of different AF ablation approaches [Narayan SM et al. J Am Coll Cardiol 2013. In press].
Sanjiv M. Narayan, MD, PhD, University of California, San Diego School of Medicine, Veterans Affairs Medical Center, San Diego, California, USA, and colleagues undertook the PRECISE-PAF trial to test their hypothesis that prospective targeted ablation of stable rotors and focal sources alone would eliminate PAF over the long term without the need for pulmonary vein isolation (PVI).
The study included 31 consecutive PAF patients undergoing FIRM-guided ablation in five centers in the United States. Patients included in the study were aged >21 years, had indications for PAF ablation, discontinued antiarrhythmics >5 half-lives, and amiodarone >30 days. The only patients excluded were those unable or unwilling to provide informed consent. The primary endpoint was single procedure freedom from AF.
Most of the study participants were male (n=28); the average age was 59 years; AF had been present for ∼4 years; the average CHADS2 score was 1.5; and 38.7% (n=12) had a CHADS2 >2. Overall, 74.2% (n=23) had hypertension and 32.3% (n=10) had coronary disease.
The primary endpoints of the study were acute elimination of diagnosed AF rotors and focal sources based on repeated mapping, as well as long-term freedom of AF (ie, using standard criteria defined as <30 seconds on external intermittent monitors or <1% in patients with continuous monitoring). Monitoring was done quarterly and antiarrhythmic drugs were discontinued after a 90-day blanking period.
For each patient, the investigators delivered FIRM-guided ablation at each source to achieve termination of AF with noninducibility or to eliminate sources on repeat FIRM-maps. Residual tachycardias were also ablated. PVI was not done.
The study found that stable rotors and focal sources arose in all 31 patients, with 2.5 AF rotor/focal sources per patient. Overall, the sources arose in the left atrium in 66.3% of the patients and in the right atrium in 33.7%.
Median FIRM-guided ablation was 17.4±8.2 minutes, and total case ablation including typical atrial flutter ablation, was a median of 22.7±9.1 minutes. Although PVI showed potential in all patients, they were not isolated.
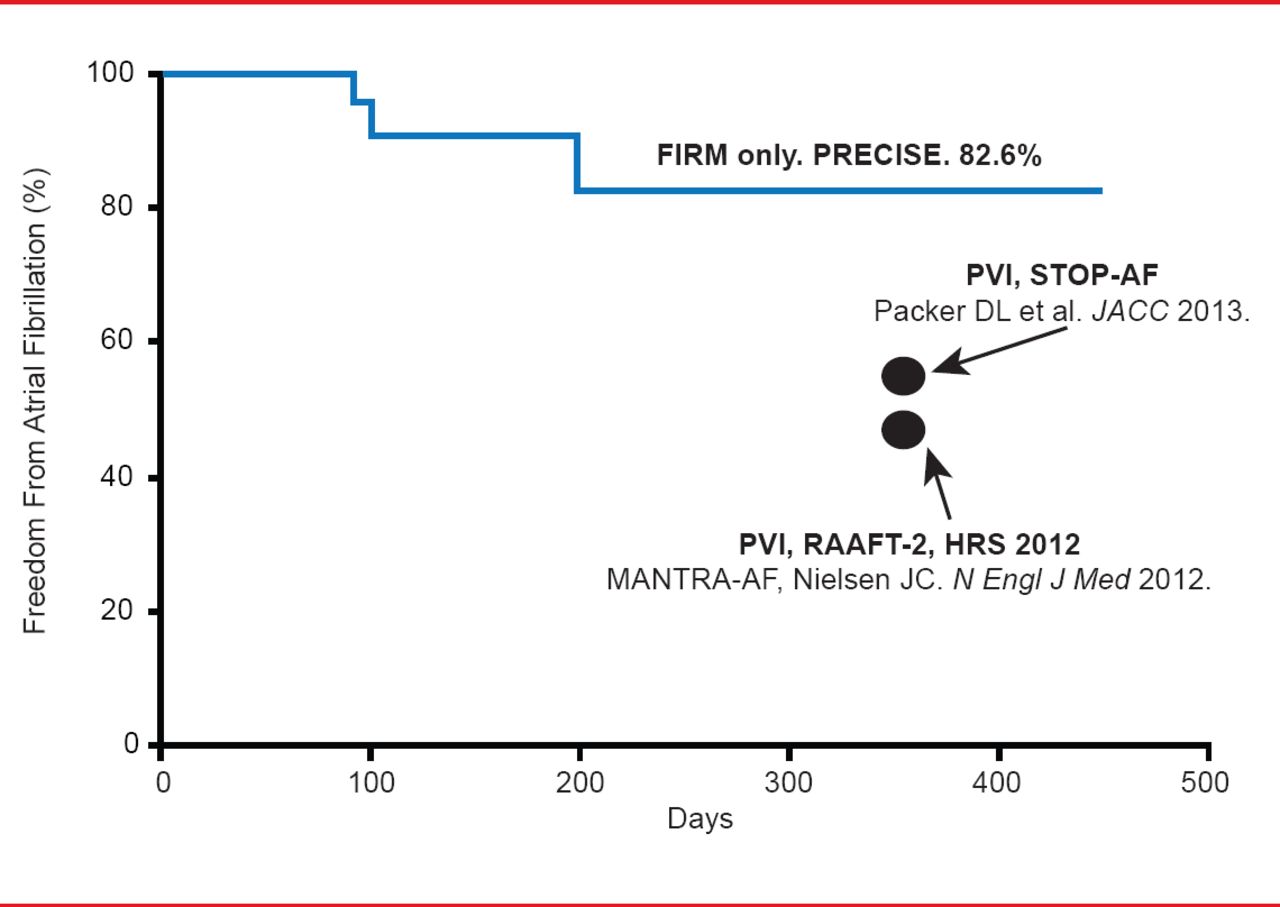
On follow-up for a median of 223 days, using more rigorous monitoring than typically used in AF trials, 82.6% of patients were free from AF after a single FIRM-guided ablation procedure. This compares favorably with the results from prior studies of PVI that provided 50% to 60% single procedure success rates (Figure 1).

Single Procedure Freedom From Atrial Fibrillation in the PRECISE-PAF Trial
Reproduced with permission from SM Narayan, MD, PhD.
Dr. Narayan concluded that the study confirms that PAF is a substrate-based disease. Accordingly, these results show that FIRM-guided ablation of stable rotors and focal sources can eliminate PAF without the need to eliminate triggers (PVI). This is in line with ablation for most other arrhythmias.
Limitations of the study highlighted by the investigators included the use of current mapping baskets that were suboptimal, the single-arm design of the study, the need for larger sample size and longer follow-up, and the focus only on PAF.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.