

Summary
Evidence From the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation trial [COMPARE; NCT01006876] confirms that the continuous use of warfarin while performing catheter ablation of AF significantly reduces the occurrence of periprocedural stroke/transient ischemic attack and bleeding complications [Di Biase L et al. Heart Rhythm 2013]. The results suggest that periprocedural anticoagulation management could play an important role in the occurrence of these complications.
- Arrhythmias
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
Evidence From the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation trial [COMPARE; NCT01006876] confirms that the continuous use of warfarin while performing catheter ablation of AF significantly reduces the occurrence of periprocedural stroke/transient ischemic attack (TIA) and bleeding complications [Di Biase L et al. Heart Rhythm 2013]. The results, presented by Luigi Di Biase, MD, PhD, Texas Cardiac Arrhythmia Institute, St. David's Medical Center, Austin, Texas, and Albert Einstein College of Medicine, at Montefiore Hospital, Bronx, New York, USA, suggest that periprocedural anticoagulation management could play an important role in the occurrence of these complications.
The open-label, randomized, parallel-group, multicenter study was conducted in 1560 patients, aged 18 to 75 years, undergoing radiofrequency catheter ablation for AF. Patients had paroxysmal, persistent, or longstanding persistent (LSP) AF; a CHADS2 score ≥1; and an international normalized ratio (INR) in the range of 2.0 to 3.0 in the last 4 to 6 weeks prior to ablation.
Group 1 patients (off warfarin; n=790) discontinued warfarin 2 to 3 days prior to ablation and bridged with low weight molecular heparin (LWMH). Heparin was given during the procedure to maintain an activated clotting time (ACT) >250 seconds. Group 2 patients (on warfarin; n=794) received warfarin therapy throughout the study as well as heparin during the entire procedure to maintain the ACT >300 seconds. Neurological and bleeding complications were assessed 48 hours after ablation in both groups. The primary endpoint was the incidence of thromboembolic events 48 hours post ablation.
Baseline characteristics were similar in both groups. LSP was present in 49% of Group 1 and 51% of Group 2 patients. CHADS2 scores ≥2 were present in 71% of Group 1 and 74% of Group 2 patients.
The incidence of periprocedural stroke was 3.7% (n=29) in Group 1: one patient with paroxysmal AF, two with persistent AF, and 26 with LSP AF. In Group 2, two (0.25%) patients experienced a stroke—both with LSP AF. The difference was significant (p<0.001). Both patients had a subtherapeutic INR the day of the procedure and no evidence of thrombus preprocedurally. When analyzing TIA and stroke together, event rates were 4.9% (n=39) in Group 1 and 0.25% (n=2) in Group 2 (p<0.001). There was no significant difference in major bleeding and pericardial effusion between the groups (Figure 1). However, significantly more Group 1 patients (22%; p<0.001) experienced minor bleeding complications compared with Group 2 (4.1%).

Periprocedural Events and Complications
TIA=transient ischemic attack.
Reproduced with permission from L Di Biase, MD, PhD.
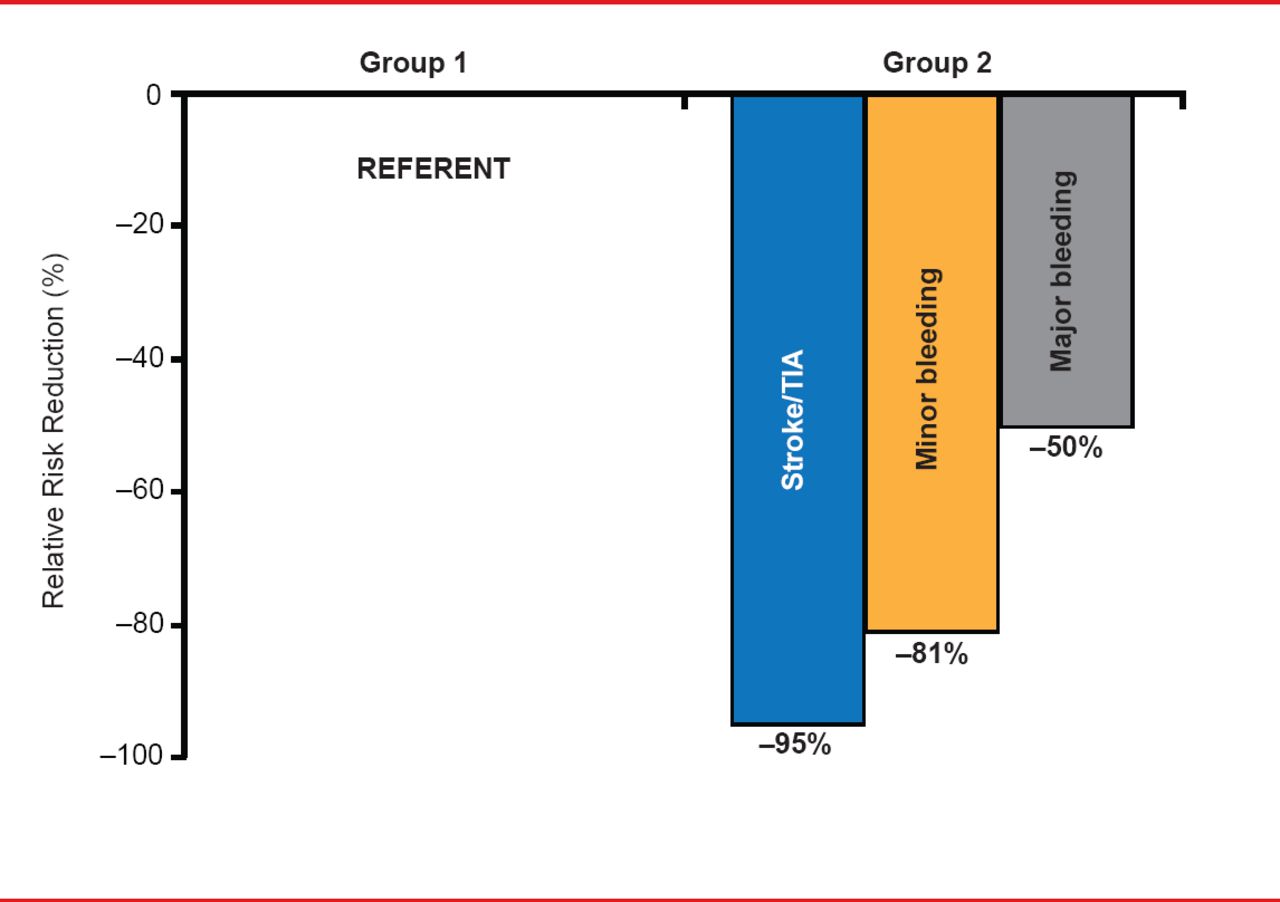
Warfarin use during ablation for AF was associated with relative risk reduction of 95% for stroke/TIA, 81% for minor bleeding, and 50% for major bleeding. Warfarin discontinuation, high CHADS2 score, and AF type (nonparoxysmal) were significant predictors of thromboembolic events (Figure 2).

Relative Risk Reduction of Periprocedural Events
TIA=transient ischemic attack.
Reproduced with permission from L Di Biase, MD, PhD.
Dr. Di Biase noted that periprocedural thromboembolic and hemorrhagic events are worrisome complications of catheter ablation for AF, particularly in patients with LSP AF, and with high CHADS2 scores [Scherr D et al. J Cardiovasc Electrophysiol 2009]. These findings support other data suggesting that the combination of an open irrigation ablation catheter and periprocedural therapeutic anticoagulation with warfarin may reduce the risk of periprocedural stroke without increasing the risk of pericardial effusion or other bleeding complications [Di Biase L et al. Circulation 2010].
Dr. Di Biase concluded that the use of the newer anticoagulants during AF ablation procedures should be investigated in these high-risk patients and only compared with strategies that did not discontinue warfarin.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.