

Summary
This article presentS new data from the Biventricular Versus Right Ventricular Pacing in Heart Failure Patients With Atrioventricular Block trial [BLOCK HF; NCT00267098], showing that biventricular (BiV) pacing is associated with better clinical outcomes, improved patient quality of life, and heart failure (HF) status. Previous reports from BLOCK HF showed that BiV pacing was superior to right ventricular pacing and led to a significant reduction in mortality, HF-related urgent care, and the risk of developing a significant increase in left ventricular end systolic volume index [Curtis AB et al. N Engl J Med 2013].
- Heart Failure
- Arrhythmias
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Heart Failure
- Arrhythmias
- Cardiology Clinical Trials
- Interventional Techniques & Devices
Anne B. Curtis, MD, University at Buffalo, Buffalo, New York, USA, presented new data from the Biventricular Versus Right Ventricular Pacing in Heart Failure Patients With Atrioventricular Block trial [BLOCK HF; NCT00267098], showing that biventricular (BiV) pacing is associated with better clinical outcomes, improved patient quality of life (QoL), and heart failure (HF) status. Previous reports from BLOCK HF showed that BiV pacing was superior to right ventricular (RV) pacing and led to a significant reduction in mortality, HF-related urgent care, and the risk of developing a significant increase in left ventricular (LV) end systolic volume index [Curtis AB et al. N Engl J Med 2013].
The current analysis assessed changes in three prespecified endpoints: Packer Clinical Composite response (determined using clinical outcomes, HF status, and patient symptoms); QoL (Minnesota Living With HF Questionnaire); and NYHA Class. The changes were measured at 6, 12, 18, and 24 months and compared with the same values measured at postimplant baseline (PIB)/randomization between the BiV and RV arms. Patients were rated as “improved,” “worsened,” or “unchanged,” and significant differences were determined by posterior probability (PP). PP values >0.95 were considered significant.
There were 349 patients in the BiV group and 342 in the RV group. Inclusion criteria included pacing indication for atrioventricular (AV) block; NYHA Class I, II, III; LV ejection fraction ≤50%; absence of a Class I indication for cardiac resynchronization therapy (CRT); and no previous pacemaker or implantable cardioverter defibrillator. Most patients were in their early 70s, had NYHA Class II or III, and second- or third-degree AV block. There were no significant differences in the results between patients implanted with CRT-P or CRT-D devices, thus these data were combined.
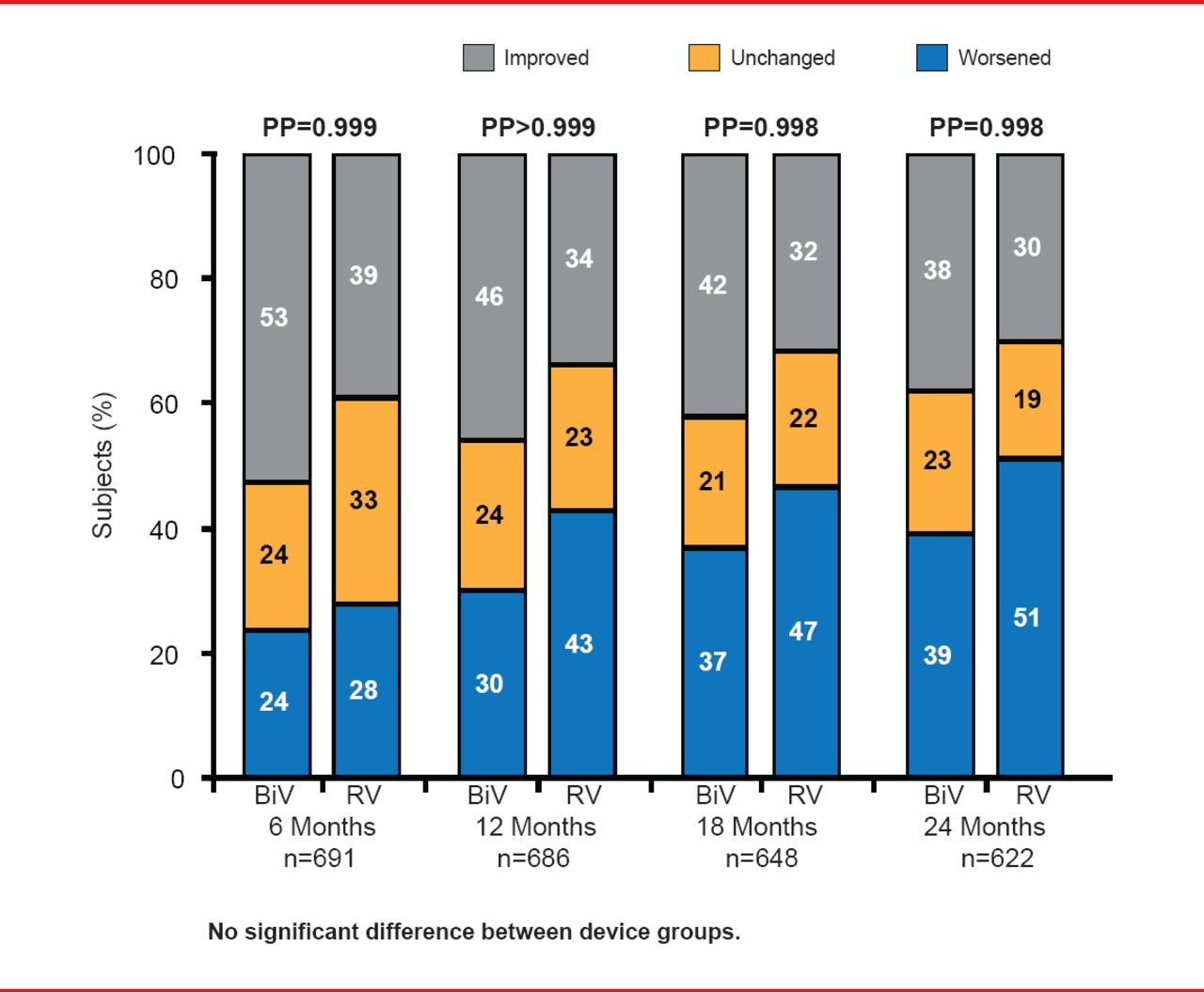
Compared with RV pacing, AV-block patients treated with BiV pacing had superior Packer Clinical Composite scores through 24 months, superior HF status as measured by NYHA class at 12 months, and superior QoL through 12 months. At every time point, significantly more patients were rated as improved on the Packer Clinical Composite score receiving BiV compared with those receiving RV pacing (Figure 1).

Packer Clinical Composite Score
BiV=biventricular; PP=posterior probability; RV=right ventricular. Reproduced with permission from AB Curtis, MD.
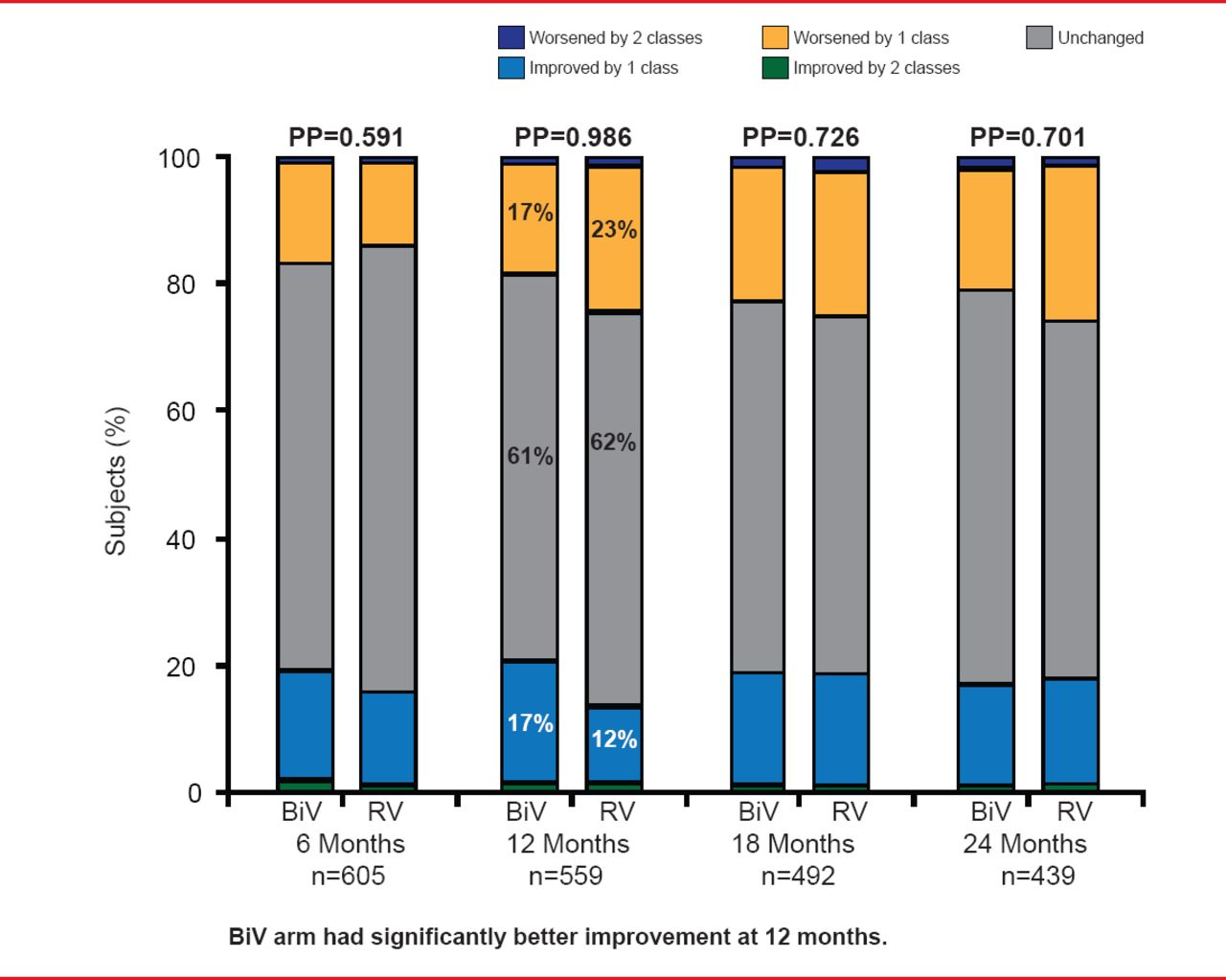
At 12 months patients in the BiV arm had significantly better improvement in NYHA class from PIB compared with RV (PP=0.986) but not at 18 or 24 months (Figure 2).

Change in NYHA Class From Postimplant Baseline
BiV=bientricular; PP=posterior probability; RV=right ventricular.
Reproduced with permission from AB Curtis, MD.
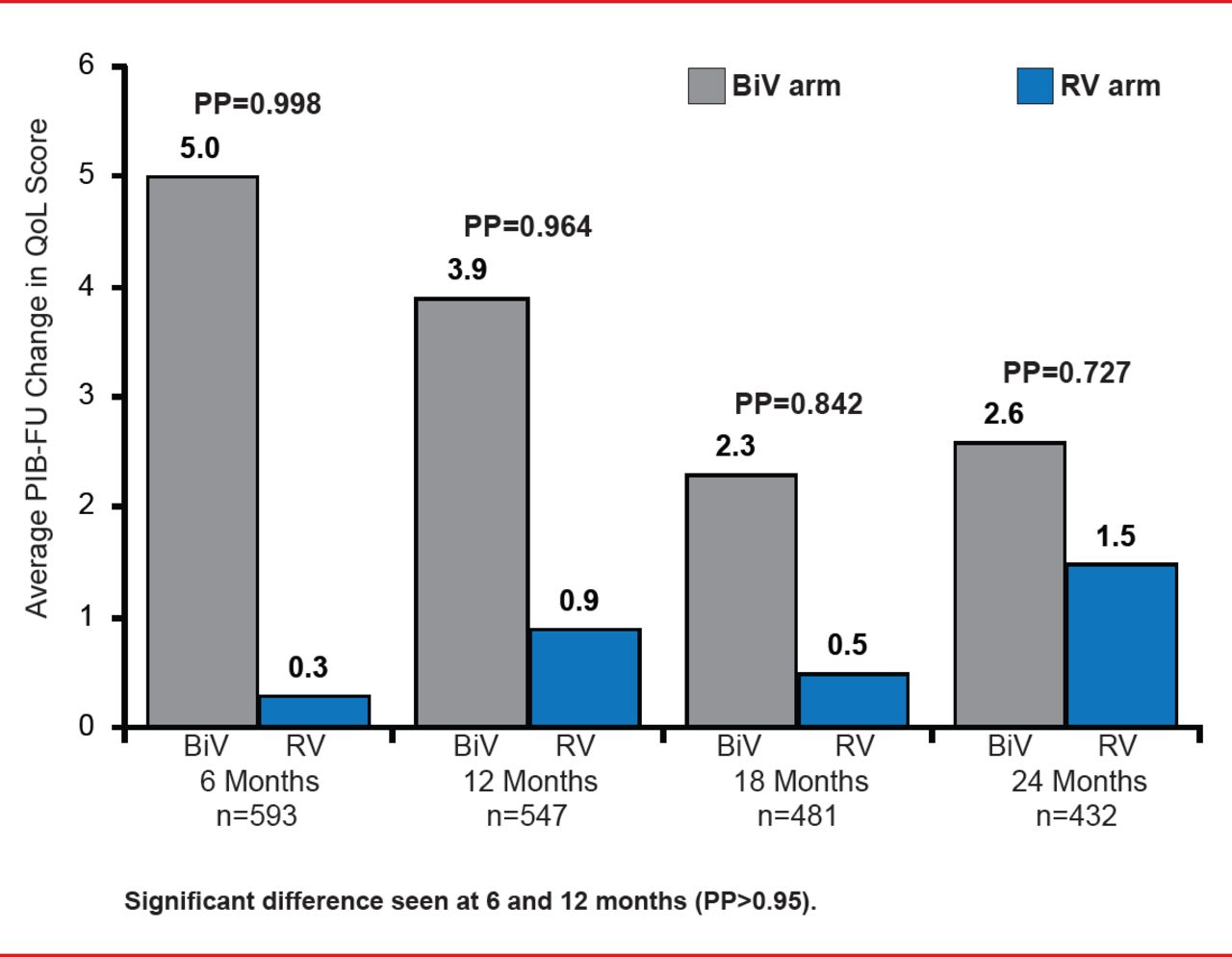
QoL was significantly improved at 6 and 12 months (PP=0998 and PP=0.964, respectively) in the BiV arm compared with the RV arm (Figure 3).

Improvement in QoL for Postimplant Baseline
BiV=biventricular; PIB-FU=postimplant baselne follow-up; PP=posterior probability; QoL=quality of life;RV=right ventricular.
Reproduced with permission from AB Curtis, MD.
Current pacing guidelines recommend permanent RV pacing for patients who develop AV block; however, clinical studies such as the Mode Selection Trial in Sinus Node Dysfunction [MOST; Lamas GA et al. N Engl J Med 2002] and Dual Chamber and VVI Implantable Defibrillator [DAVID; Wilkoff BL et al. JAMA 2002] trials have shown that RV pacing may have long-term deleterious effects such as increased risk of HF hospitalization and LV systolic dysfunction.
Dr. Curtis concluded, “For patients with AV block and systolic dysfunction, biventricular pacing not only reduces the risk of mortality and morbidity, but also leads to better clinical outcomes and improved patient quality of life and heart failure status.”
NOTE: The use of CRT devices for AV block and systolic dysfunction patients without ventricular dyssynchrony is not approved in the United States.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.