

Summary
This article provides an overview of emerging pharmacotherapies for the treatment of diabetic retinopathy (DR). Specific topics include laser treatment, the targeting of vascular endothelial growth factor, steroid therapy, and other current approaches for DR therapy.
- Retinal Diseases
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
- Retinal Diseases
- Diabetes Mellitus
Arup Das, MD, PhD, University of New Mexico School of Medicine, Albuquerque, New Mexico, USA, provided an overview of emerging pharmacotherapies for the treatment of diabetic retinopathy (DR). In the late 1980s it was determined that microaneurysms, the earliest clinical lesions of DR, occur due to loss of pericytes that, in turn, spur endothelial cell proliferation in the eye [Kelly C et al. J Cell Biol 1987; Orlidge A, D'Amore PA. J Cell Biol 1987; Das A et al. Exp Eye Res 1988]. Nonproliferative DR includes diabetic macular edema (DME), with the hallmark of hard exudates, edema, and hemorrhage.
The cell proliferation (angiogenesis) that occurs in proliferative diabetic retinopathy (PDR) has been hypothesized to result from the hypoxia that can occur during advanced stages of the disease. The resulting elaboration of angiogenic factors, such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor, and insulin-like growth factor, spurs vessel formation in the eye. These new vessels result in vitreous hemorrhage and sometimes traction retinal detachment, causing severe visual loss.
LASER TREATMENT
The current standard treatment for PDR is panretinal laser photocoagulation (PRP). Untreated eyes incur more severe visual loss than laser-treated eyes as shown by the DR study.
While PRP laser treatment has undisputed benefits in eyes with PDR, potential complications include loss of peripheral vision and loss of night vision [Bressler NM et al. N Engl J Med 2011]. A clinical trial is under way to examine whether anti-VEGF injections are more beneficial than the current PRP laser treatment.
TARGETING OF VEGF
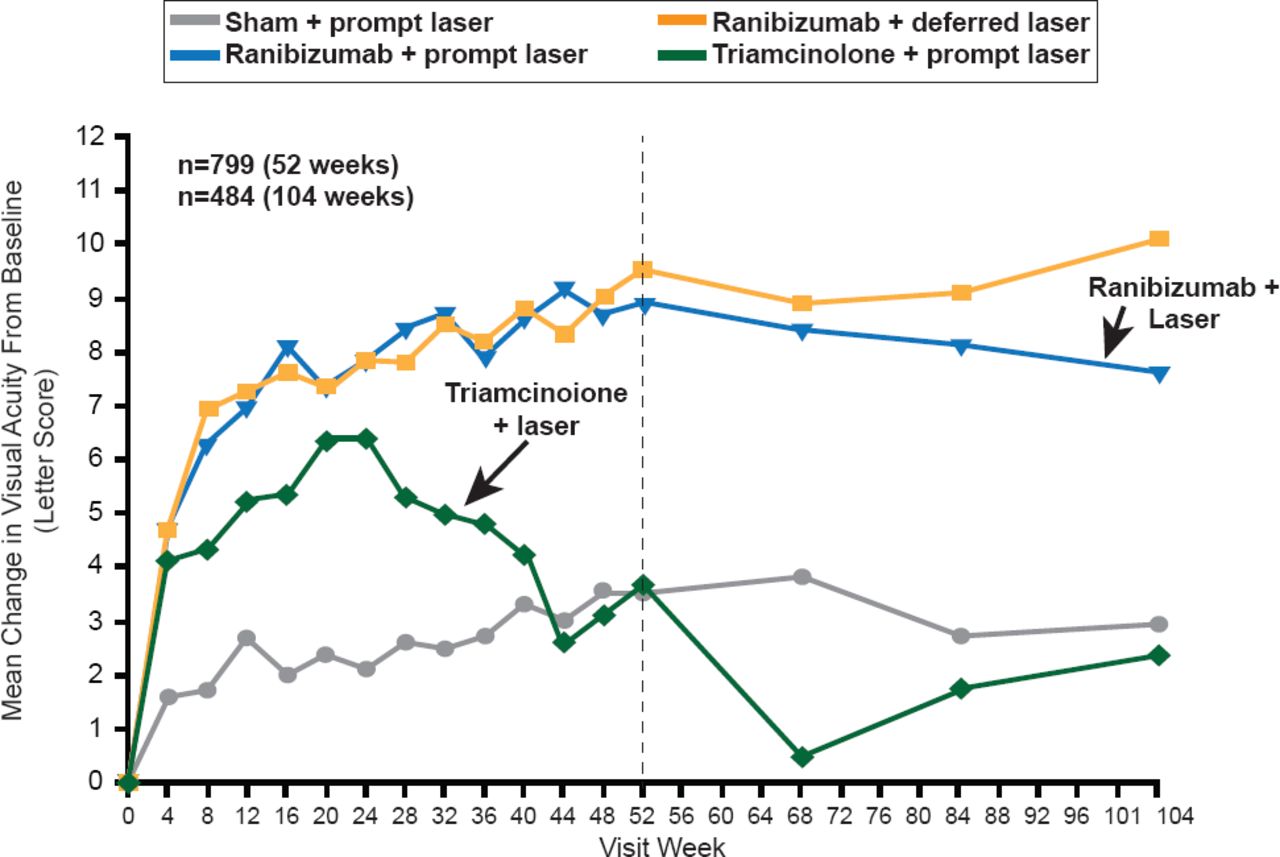
A more recent approach has been the targeting of VEGF, which is upregulated in DME, particularly in extensive DME [Funatsu H et al. Ophthalmology 2003]. Trials of various VEGF- targeted approaches, including monoclonal antibodies (pegaptanib, bevacizumab, ranibizumab, VEGF trap), have yielded encouraging results (Figure 1; Table 1) [Elman M et al. Ophthalmology 2010]. However, ranibizumab is the only Food and Drug Administration-approved drug now for treatment of DME.
Diabetic Retinopathy Trials With Anti-VEGF Agents

Ranibizumab in Diabetic Macular Edema: DRCR Protocol I
Reproduced from Elman M et al. Randomized Trial Evaluating Ranibizumab Plus Prompt or Deferred Laser or Triamcinolone Plus Prompt Laser for Diabetic Macular Edema. Opthalmology 2010;117(6)1604–1077. With permission from Elsevier.
Particularly for center-involved DME, the consensus is that anti-VEGF strategies slow disease progression, reverse features of DR, and delay the need for laser treatment. However, residual macular edema is problematic. Several intravitreal anti-VEGF injections are necessary to treat DME, and the effect of these drugs are not as robust as they are in PDR. Furthermore, targeted, chronic obliteration of VEGF may be toxic, triggering the death of cone receptors required for central and color vision [Kurihara T et al. J Clin Invest 2012].
STEROID THERAPY
The use of steroids to relieve inflammation that can exacerbate DME is an attractive approach. The two recent randomized, double-masked, parallel-group, multicenter Fluocinolone Acetonide for Macular Edema studies [FAME; NCT00502541, NCT00576459] have been particularly noteworthy. Nonbiodegradable cylindrical implants harboring fluocinolone acetonide were inserted into patient eyes. The primary outcome (improved vision of >15 letters) was achieved by 29% of the collective patients at 3 years versus 19% for the sham group. Patients with a longer history of DME showed a greater benefit. Yet, 89% of treated patients required cataract surgery and up to ∼2% required trabeculoplasty (Food and Drug Administration approval awaiting additional data).
OTHER APPROACHES
Angiopoietin 2 is another potential target for DME. This proinflammatory cytokine has been linked with increased vascular permeability in DME. Nonsteroidal anti-inflammatory drugs may have therapeutic value. High daily doses of aspirin may slow the development of retinal microaneurysms, although this conclusion is equivocal. Tumor necrosis factor-α is another proinflammatory cytokine that had reported value in DME in a small Phase 3 trial [Sfikakis PP et al. Diabetes Care 2010]. Other potential targets include chemokines like CCL2, and kallikrein-kinin system.
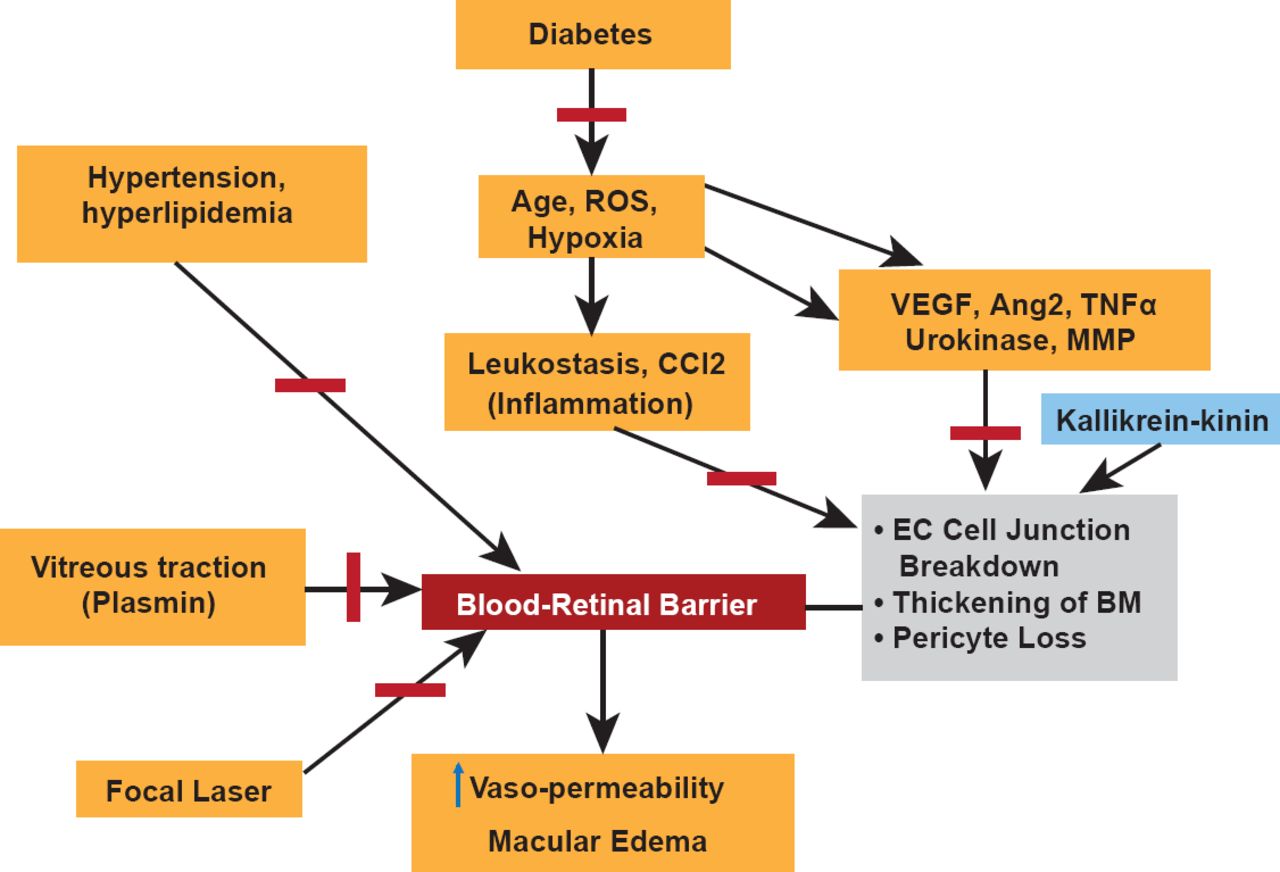
DME involves a complex interplay of a variety of risk factors and molecular pathways (Figure 2). Research over the past 3 decades has considerably clarified the picture. But, more remains to be done, particularly concerning the therapeutic tools and their optimal concentrations.

Summary of Factors Important in DME
BM=basement membrane; EC=endothelial cell; MMP=matrix metalloproteinases; ROS=reactive oxgen species; TNF-α=tumor necrosis factor-α; VEGF=vascular endothelial growth factor.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.