

Summary
Patients with structural heart disease (SHD) who experience sustained monomorphic ventricular tachycardia (SMVT) are usually considered to have a poor prognosis. This article discusses the results of the Radio-Frequency Ablation as a primary management for Sustained Monomorphic Ventricular Tachycardia in Patients With Structural Heart Disease (ie, without implantation of a defibrillator). The investigators hypothesized that these patients would have a favorable prognosis and that any recurrences would not result in death.
- Interventional Radiology
- Cardiology Clinical Trials
- Arrhythmias
- Interventional Techniques & Devices
- Interventional Radiology
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Arrhythmias
- Interventional Techniques & Devices
Patients with structural heart disease (SHD) who experience sustained monomorphic ventricular tachycardia (SMVT) are usually considered to have a poor prognosis. According to the American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Rhythm Society (HRS) 2008 Guidelines for device-based therapy of cardiac rhythm abnormalities, therapy with an implantable cardioverter defibrillator (ICD) is indicated in patients with SMVT and SHD [Epstein AE et al. Circulation 2008]. The ACC/AHA/European Society of Cardiology (ESC) 2006 Guidelines recommend ablation for patients with SMVT who are at low risk for sudden cardiac death (SCD) [Zipes DP et al. Circulation 2006]. a condition which “a priori” does not correspond to patients with structural heart disease.
Philippe Maury, MD, University Hospital Rangueil, Toulouse, France, reported the results of the Radio-Frequency Ablation as a primary management for Sustained Monomorphic Ventricular Tachycardia in Patients With Structural Heart Disease (ie, without implantation of a defibrillator). The investigators hypothesized that these patients would have a favorable prognosis and that any recurrences would not result in death.
The study included 166 consecutive patients with SHD treated with radiofrequency ablation (RFA) without an ICD for well-tolerated SMVT, defined as a lack of syncope or cardiac collapse at the time of VT and an ejection fraction (EF) >30%. The control group consisted of patients from the Antiarrhythmics Versus Implantable Defibrillators registry [AVID; Raitt MH et al. Circulation 2001].
Of the 166 patients, 93 (56%) presented with palpitations only, 35 (21%) with presyncope, 24 (14%) with congestive heart failure, and 15 (9%) with chest pain. A total of 187 ablations were performed. Following ablation, VT was not inducible in 137 of 158 patients (87%), while 21 patients (13%) had inducible VT (6 clinical, 15 nonclinical). Complications occurred in 11 patients (6.5%), including pericardial effusion (n=1), tamponade (n=3), groin hematoma (n=4), femoral pseudo-aneurysm (n=1), and atrioventricular block (n=2). There were no deaths directly related to the procedure. At discharge, patients were prescribed β-blockers (43%), amiodarone (5%), amiodarone plus a β-blocker (17%), sotalol (10%), a Class 1 antiarrhythmic (3%), or no drug (22%).
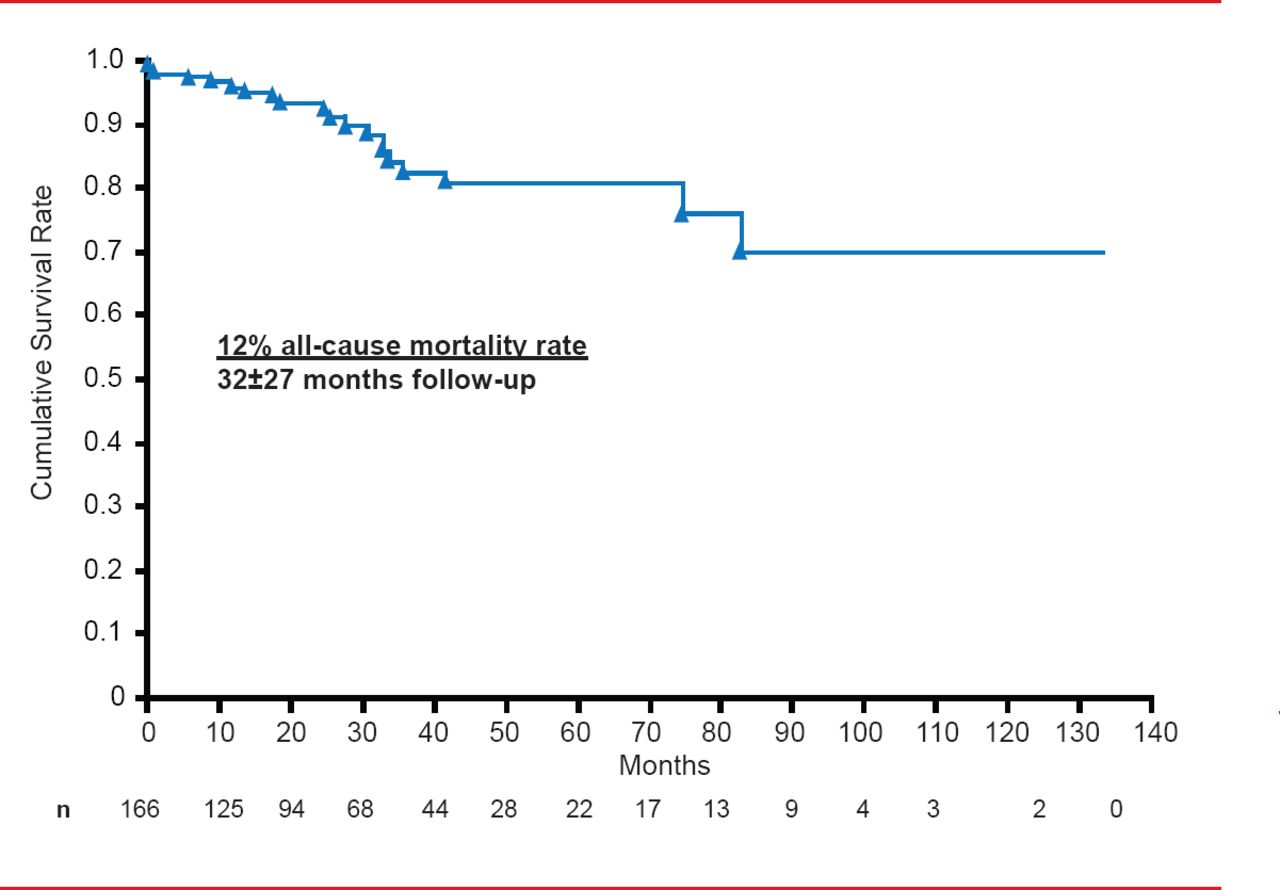
At a follow-up of 32±27 months, 20 patients (12%) had died (4.5% annual rate), including 8 (40%) noncardiovascular deaths, 4 (20%) sudden deaths, and 8 (40%) nonarrhythmic cardiovascular deaths (Figure 1). The cumulative sudden death rate was 2.4%. None of the patients who died suddenly had recurrent VT before death.

Cumulative Survival at 32±27 Months Follow-Up
Reproduced with permission from P Maury, MD.
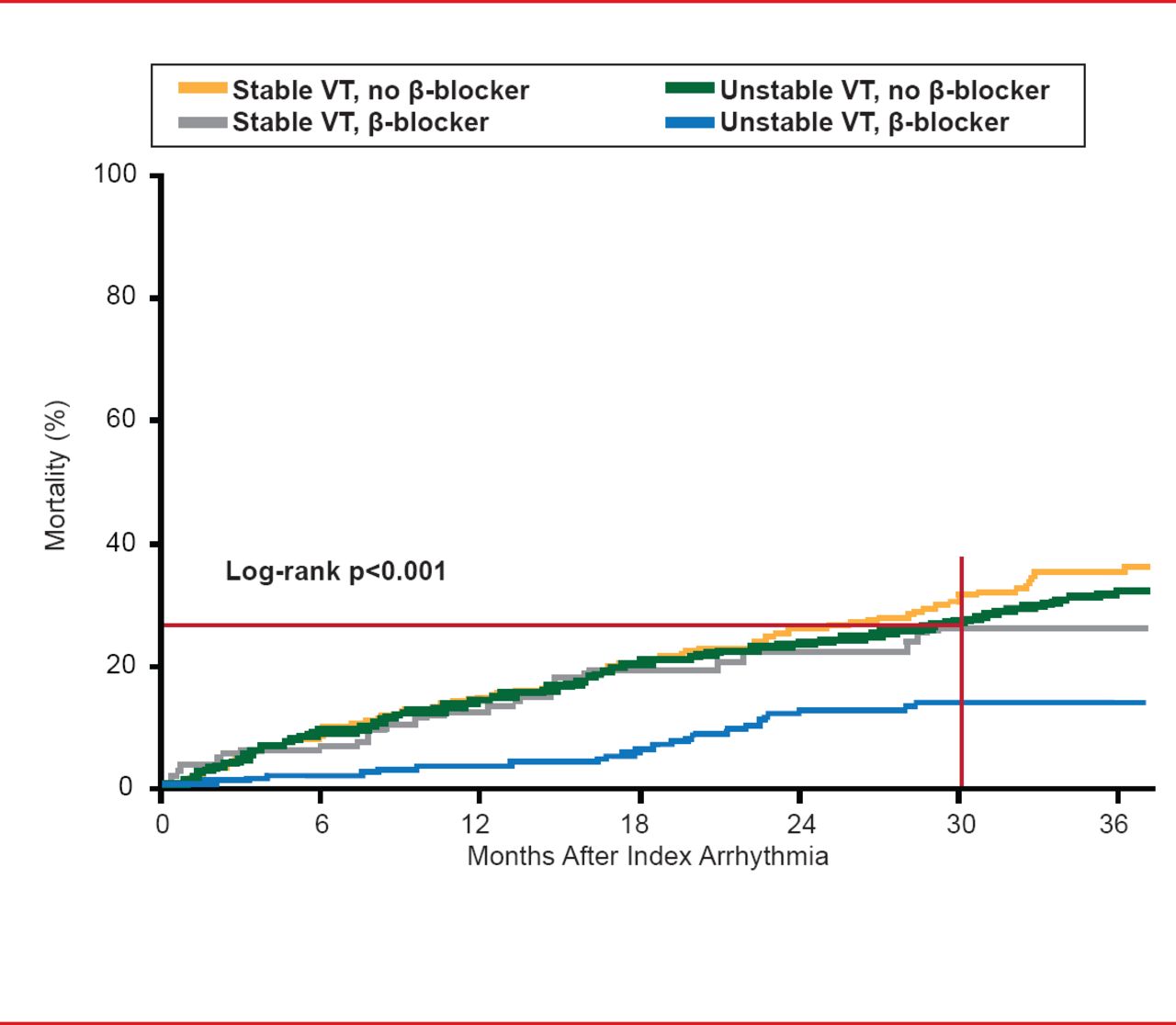
In comparison, 30-month all-cause mortality in the similar patients from the AVID trial control group [Raitt MH et al. Circulation 2001] was >20% (Figure 2).
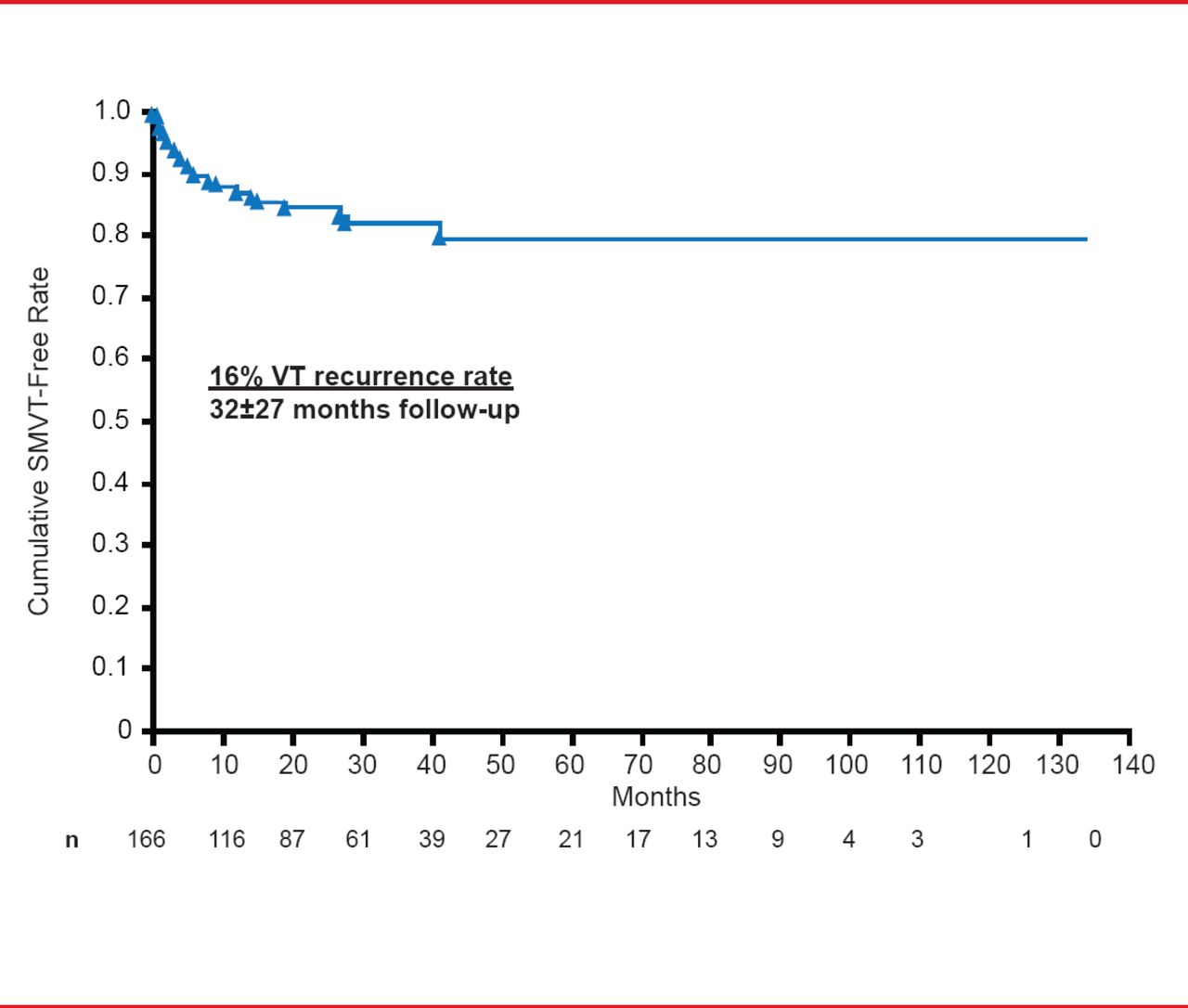
During follow-up, 27 patients (16%) had recurrent VT (6% annual rate; Figure 3). Among these patients, 5 had received an ICD only, 14 had ablation (followed by an ICD in 6 of 14), and 8 did not have ablation or an ICD.

AVID Registry All-Cause Mortality at 30 Months
VT=ventricular tachycardia.
Reproduced with permission from P Maury, MD.

Cumulative SMVT-Free Rate at 32±27 Months
SMVT=sustained monomorphic ventricular tachycardia; VT=ventricular tachycardia.
Reproduced with permission from P Maury, MD.
Prof. Maury concluded that primary RFA for well-tolerated SMVT in patients with SHD and non severely depressed EF, without ICD implantation, is effective and is not associated with a significant risk of late sudden death. However, this was a retrospective multicenter study with a variety of ablation procedures and endpoints, and with a mean follow-up of only 30 months. Prospective randomized trials are needed to evaluate RFA versus ICD in patients with SHD and SMVT.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.