

Summary
The risk of recurrent venous thrombosis (VT) is higher than for a first event, thus prevention is even more relevant. This article discusses paradoxes and the risk factors for recurrent VT including thrombophilia, clinical presentation with primary deep vein thrombosis (DVT), shorter duration of anticoagulation, and increasing age [Prandoni P et al. Haematologica 2007]. Also discussed is the optimal treatment duration to avoid VTE recurrence and risk stratification models to predict risk or recurrent VTE [Prandoni P et al. Haematologica 2007].
- Thrombophilia
- Thrombotic Disorders
- Thrombophilia
- Hematology
- Thrombotic Disorders
The risk of recurrent venous thrombosis (VT) is higher than for a first event, thus prevention is even more relevant. Suzanne Cannegieter, MD, Leiden University Medical Center, Leiden, The Netherlands, discussed paradoxes and the risk factors for recurrent VT including thrombophilia, clinical presentation with primary deep vein thrombosis (DVT), shorter duration of anticoagulation, and increasing age [Prandoni P et al. Haematologica 2007].
Important concepts in the prevention of recurrent VT include the recognition that the causes of VT differ between individuals, there are different types of risk factors, and the risk profile for recurrence is different from that of a first event. The thrombosis potential model developed by Rosendaal [Lancet 1999] can be used to indentify high-risk groups, different types of risk factors, and why certain individuals develop thrombosis at specific points in time.
Paradoxically, although thrombophilia is a significant predictor of a first thrombotic event, it is not a predictor of recurrent events. Thus testing for heritable thrombophilia or prothrombotic defects does not add any strategic information for prevention of a recurrent venous thromboembolism (VTE). Patients whose initial thrombotic event is idiopathic have a higher risk of a second thrombotic event than patients whose initial event is provoked (HR, 1.9; 95% CI, 1.2 to 2.9) [Christiansen SC et al. JAMA 2005]. Clinical risk factors, on the other hand, do predict the risk of recurrence in that patients with postoperative VTE have a very low rate of recurrence [Baglin T et al. Lancet 2003].
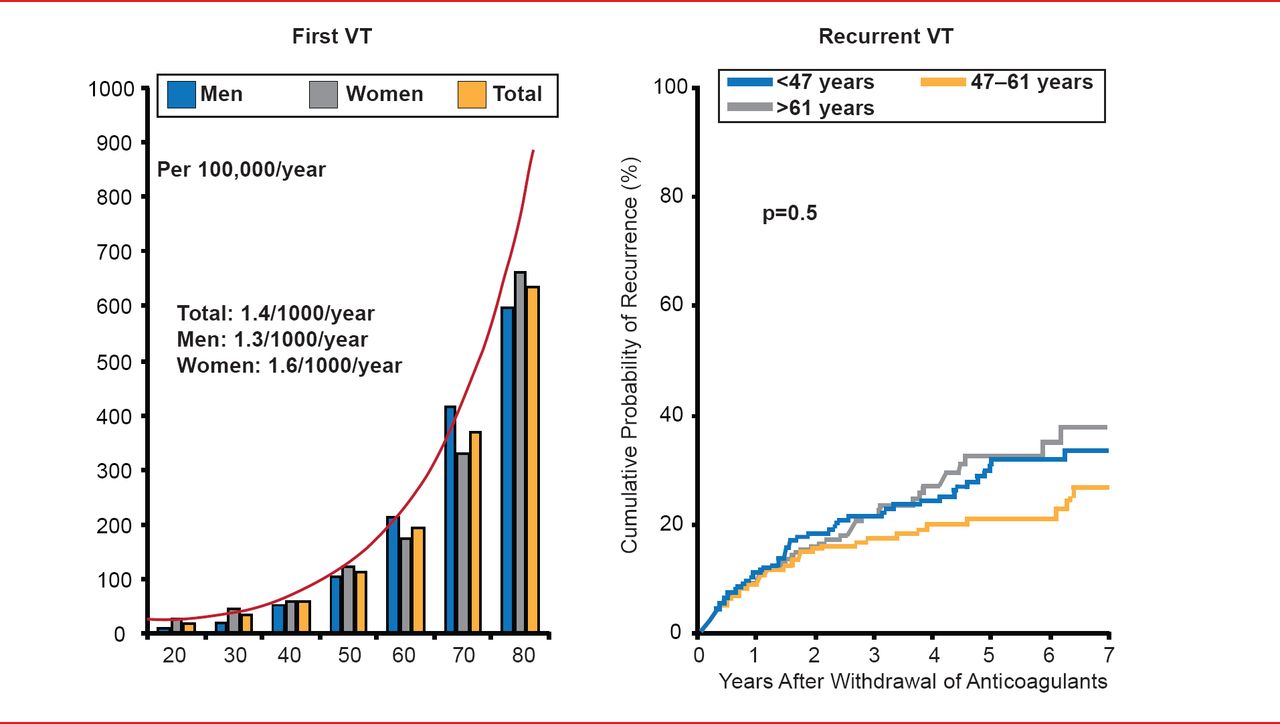
Although the incidence rates of first VT increase exponentially with age, and are slightly higher in women than in men, [Naess IA et al. J Thromb Haemost 2007] age does not play a role in recurrent VT (Figure 1) [Eischer L et al. Medicine (Baltimore) 2009; Flinterman LE et al. In preparation].

Effect of Age on Recurrent VT
Reproduced from Naess AI et al. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost 2007;5(4):692–699. With permission from the International Society of Thrombosis and Haemostasis
Reproduced from Eischer L et al. Age at First Venous Thromboembolism and Risk of Recurrence: A Prospective Cohort Study. Medicine (Baltimore) 2009;88(6): 366–370. With permission from Lipincott, Williams, and Wilkins.
Unlike first events, in which the differences between men and women are small, the incidence of recurrence is significantly (p<0.001) higher in men [Kyrle PA et al. N Engl J Med 2004] who seem to have a 50% higher risk of recurrent VTE after stopping anticoagulant treatment versus women [McRae S et al. Lancet 2006].
TYPES OF RISK FACTORS
Different transient risk factors can identify which patients should undergo short-term versus indefinite treatment. In general, recurrent risk is low when a transient risk factor was present at the first event. The risk reduction is related to the strength of the transient risk factor. For example, surgery is a strong risk factor for VT, but the risk of recurrence is low if VTE was provoked by surgery, intermediate if provoked by a nonsurgical risk factor, and high if unprovoked (Figure 2) [Iorio A et al. Arch Intern Med 2010].

Transient Risk Factors
Adapted from Iorio A et al. Arch Intern Med 2010;170(19):1710.
Although they remain causes of recurrence, fixed risk factors (age, genetic thrombophilia) play no role in predicting subsequent recurrence once the thrombotic threshold is reached.
Progressive risk factors such as cancer malignancy [Prandoni P et al. Blood 2002], inflammatory bowel disease [Novacek G et al. Gastroenterology 2010], and increasing BMI [Eichinger S et al. Arch Intern Med 2008] do appear to be connected to recurrent VT and the amount of risk is associated with the strength of the risk.
New transient risk factors after a first event including hormone use, pregnancy, surgery, plaster cast, and air travel can increase the risk of VT recurrence 4- to 25-fold [Christiansen SC et al. J Thromb Haemost 2010]. If possible, exposure to these risk factors after a first event should be avoided, and if this is not possible, thromboprophylaxis is warranted.
Markers of the thrombogenic process (D-dimer, high levels of FVIII, thrombin generation levels, residual thrombois, and proximal or distal first event) may not be true causes but are good predictors of a low risk recurrence.
With respect to prevention, patients who have strong transient risk factors at the time of their first event are at low risk, while patients exposed to new transient risk factors are at higher risk of a second VT. Patients who are exposed at the time of their first event to progressive risk factors are at high risk of a second VT, while in patients in whom none of the above risk factors were present at the time of their first event and who have only fixed risk factors, efforts must be made to distinquish higher from lower risk by means of a highly-detailed risk profile.
VTE is a common and chronic disease with a considerable risk of recurrence. Patients with acute unprovoked (idiopathic) deep vein thrombosis (DVT) or pulmonary embolism (PE) have a higher risk of VTE than patients with secondary thrombosis. Walter Ageno, MD, University of Insubria, Varese, Italy, discussed the optimal treatment duration to avoid VTE recurrence and risk stratification models to predict risk or recurrent VTE [Prandoni P et al. Haematologica 2007].
The risk of recurrent VTE is low (0.7% per patient year) if provoked by surgery, intermediate (4.2%) if provoked by a nonsurgical risk factor, and high (7.4%) if unprovoked. The risks for unprovoked VTE are common among middle-aged patients, in men in general, and in patients presenting with DVT [Prandoni P et al. Haematologica 2007; Ageno W et al. Intern Emerg Med 2011]. The risk effect can be used to determine whether patients should undergo short or indefinite treatment [Iorio A et al. Arch intern Med. 2010]. Patients are usually protected from recurrent VTE while on anticoagulation therapy, but the risk increases when therapy is stopped. For low-risk patients, 3 months of treatment is usually sufficient, while longer treatment durations do not appear to improve protection (1.5 months vs longer durations: HR, 1.52; 95% CI, 1.14 to 2.02; 3 months vs longer duration: HR, 1.19; 95% CI, 0.86 to 1.65) [Boutitie F et al. BMJ 2011].
Patients with unprovoked VTE, active cancer, or previous VTE have a risk of recurrence as high as 30% within 5 years after cessation of anticoagulation and a high case-fatality rate. Thus, 3 months of treatment may not be enough for these patients and indefinite anticoagulation treatment should be considered.
However, anticoagulation confers a considerable risk of bleeding and clinicians need to identify those patients who will not benefit from indefinite anticoagulation [Linkins LA et al. Ann Intern Med 2003]. Risk can vary depending on other factors such as age, presence of previous bleeding, cancer, renal failure, diabetes, and recent surgery.
Besides alternative treatment strategies (rivaroxaban, dabigatran, apixaban) to improve safety, clinicians are working to develop risk assessment tools. Tools that take into consideration concurrent clinical characteristics, location of first event, gender, obesity, positive D-dimer, residual vein obstruction, post-thrombotic syndrome, and thrombophilia have been shown to have predictive possibility. Risk stratification models to identify intermediate risk patients who can safely discontinue treatment at 3 months and bleeding risk assessment tools are also needed.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.