

Summary
The characteristics, management, and outcomes of outpatients with stable coronary artery disease are being studied in the multicenter Prospective Observational Longitudinal Registry of Patients with Stable Coronary Artery Disease [CLARIFY; ISRCTN43070564]. This article discusses data on the prevalence of angina and myocardial ischemia in this cohort and their association with clinical outcomes.
- Cardiology Clinical Trials
- Coronary Artery Disease
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Coronary Artery Disease
The characteristics, management, and outcomes of outpatients with stable coronary artery disease (CAD) are being studied in the multicenter Prospective Observational Longitudinal Registry of Patients with Stable Coronary Artery Disease [CLARIFY; ISRCTN43070564]. Philippe Gabriel Steg, MD, University of Paris, Paris, France, presented data on the prevalence of angina and myocardial ischemia in this cohort and their association with clinical outcomes. He noted that little information is available in the current era of widespread revascularization and increased utilization of effective medical therapies (eg, β-blockers, statins).
The CLARIFY registry provides a dataset of 32,396 patients with stable CAD with at least one of the following at the time of enrollment: prior myocardial infarction (MI), chest pain and evidence of myocardial ischemia, evidence of CAD on coronary angiography, and prior percutaneous coronary intervention or coronary artery bypass surgery. All patients were enrolled in 2009 or 2010 across 45 countries and now have at least 2 years of follow-up.
The present analysis found that 20,402 (63%) of these CLARIFY patients underwent a noninvasive test for myocardial ischemia within 12 months prior to enrollment that did not lead to revascularization. Baseline data was used to characterize these patients as having neither angina nor ischemia (n=13,283), angina but no ischemia (n=1843), ischemia but no angina (n=3060), and both angina and ischemia (n=2216). Approximately two thirds of these patients had neither angina nor ischemia.
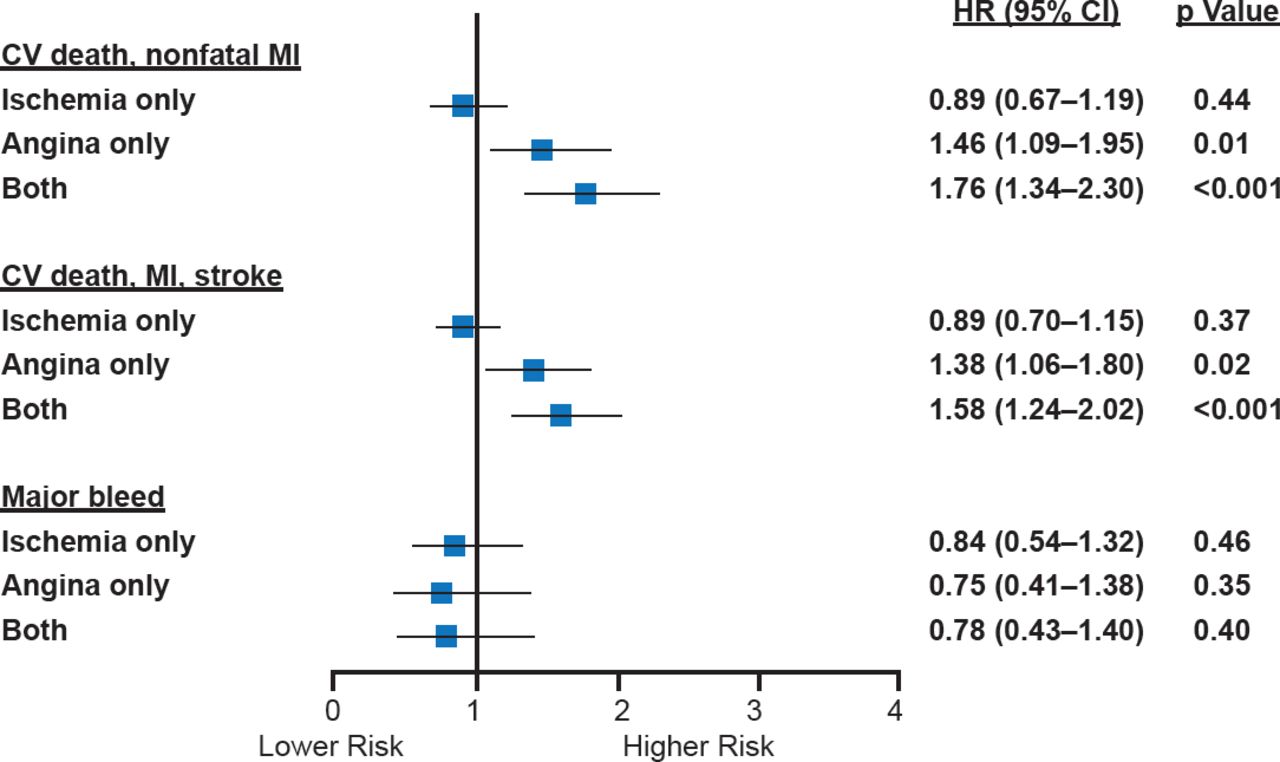
There was no difference in the primary composite endpoint of cardiovascular death and nonfatal MI between patients with ischemia alone versus those without ischemia and angina (HR, 0.89; Figure 1). Those with angina alone did have an increased risk (HR, 1.46; 95% CI, 1.09 to 1.95) and those with both angina and ischemia appeared to have an even higher risk (HR, 1.76; 95% CI, 1.34 to 2.30).

Outcomes by Ischemia or Angina Status in CLARIFY
CV=cardiovascular; MI=myocardial infarction.
*All outcomes were adjusted for age, sex, geographical region, smoking status, hypertension, dyslipidemia, and diabetes.
Reproduced with permission from PG Steg, MD.
Although the majority of stable CAD outpatients have neither angina nor ischemia, the presence of both appeared to confer higher risk for all of the cardiovascular secondary endpoints. Prof. Steg noted that 60% of the events in this dataset occurred in the subgroup with neither angina nor ischemia at baseline, emphasizing the need to optimize secondary prevention measures even in stable, asymptomatic patients.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.