

Summary
New guidelines have been issued by the European Society of Cardiology and partnering organizations for the management of stable coronary artery disease; diabetes, prediabetes, and cardiovascular disease; cardiac pacing and cardiac resynchronization therapy, and arterial hypertension.
- Coronary Artery Disease
- Interventional Techniques & Devices Hypertensive Disease
- Arrhythmias
- Cardiology Guidelines
- Diabetes Mellitus
- Coronary Artery Disease
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Hypertensive Disease
- Arrhythmias
- Exclusive Article - For home page
- Cardiology Guidelines
- Diabetes Mellitus
New guidelines have been issued by the European Society of Cardiology (ESC) and partnering organizations for the management of stable coronary artery disease (CAD); diabetes, prediabetes, and cardiovascular disease (CVD); cardiac pacing and cardiac resynchronization therapy (CRT), and arterial hypertension.
STABLE CORONARY ARTERY DISEASE
Gilles Montalescot, MD, PhD, Pitié-Salpétrière Hospital, Paris, France, and Udo Sechtem, MD, Robert-Bosch Hospital, Stuttgart, Germany, presented an overview of the new ESC guidelines for the management of stable CAD [Montalescot G et al. Eur Heart J 2013]. These updated guidelines gave added prominence to modern imaging techniques such as CV magnetic resonance imaging and coronary computed tomography angiography (CCTA) for use in the diagnosis of CAD. Additionally, the diagnostic algorithm of patients with suspected CAD is now based on the pretest probability of chest pain being related to CAD. Patients at high pretest probability of CAD, defined as >85%, do not need to undergo a battery of tests before being directed to invasive coronary angiography.
In order to prevent the overuse of CCTA, the guidelines define which patients should receive CCTA. CCTA is most helpful in patients at the lower range of intermediate pretest probabilities (an intermediate pretest probability is considered 15% to 85%) as a noninvasive technique to exclude coronary stenoses.
The guidelines focus on the need to control heart rate in patients being treated medically for stable angina. β-blockers or heart rate-lowering calcium channel blockers remain the first-line therapy to achieve this goal. Second-line treatment includes long-acting nitrates and the newer agents such as ivabradine, nicorandil, ranolazine, and trimetazidine.
As in the 2006 guidelines, revascularization was recommended for patients at high risk for coronary events, defined as an estimated annual mortality ≥3% or angina refractory to medical therapy. Before any discussion about revascularization, patients should receive optimal medical therapy. Moreover, revascularization should only be considered in patients with evidence of regional ischemia as assessed by either perfusion imaging or fractional flow reserve, said Prof. Montalescot.
DIABETES, PREDIABETES, AND CARDIOVASCULAR DISEASES
Lars Rydén, MD, Karolinska Institute, Stockholm, Sweden, and Peter J. Grant, MD, University of Leeds, Leeds, United Kingdom, presented the new guidelines on diabetes, prediabetes, and CVD. Produced by the ESC in collaboration with the European Association for the Study of Diabetes, these new guidelines introduce a new recommendation that endorse the use of HbA1C levels in the diagnosis of diabetes [Rydén L et al. Eur Heart J 2013]. If either HbA1C or fasting plasma glucose is elevated, the patient is diagnosed with diabetes. If there is strong suspicion that the patient has diabetes but the diagnosis is in doubt (eg, HbA1C or fasting plasma glucose is not elevated), an oral glucose tolerance test may be appropriate, said Prof. Rydén.
CV risk assessment has been simplified in the guidelines, and risk scores are no longer utilized to categorize people as having low, moderate, high, or very high risk for CVD. Patients with diabetes are considered to be at high risk for the development of CAD and CV events. In addition, patients with diabetes and CVD (eg, myocardial infarction, angina pectoris, or peripheral vascular disease) are at very high risk of recurrent CV events.
Recommendations on revascularization have undergone two major changes. In patients with stable CAD and no complex coronary lesions, medical therapy is recommended before revascularization unless there are large areas of ischemia or significant stenosis in either the left main or proximal left anterior descending artery. Also, bypass surgery is preferable in patients with diabetes who have complex coronary artery stenoses or elevated SYNTAX scores.
Multifactorial medical management is endorsed, including combinations of blood pressure-lowering agents that incorporate blockers of the renin-angiotensin-aldosterone system (RAAS), statins for the control of lipids, antiplatelet therapy, and a combination of glucose-lowering therapies. Aspirin is not recommended for the primary prevention of CV events in patients with diabetes who are at low risk of CV events. Aspirin is indicated for secondary prevention in patients with diabetes. Additionally, patients with diabetes who have an acute coronary syndrome should be treated with a P2Y12 receptor blocker (preferably prasugrel or ticagrelor) for 1 year.
Prof. Grant then explained that glycemic control should be individualized (Table 1) based on the patient. HbA1C should continue to be used to determine the need for intensification of diabetes control. The target HbA1C is lower (≤7.0%) in young patients recently diagnosed with diabetes who have no known CVD. The target HbA1C should be higher (7.5% to 8.0%) in older patients with long-standing diabetes and CV complications in order to avoid adverse events related to hypoglycemia.
Glycemic Control: Individualized Care
The general blood pressure (BP) target for patients with diabetes is <140/85 mm Hg. In patients who also have evidence of renal dysfunction, the target BP is <130/85 mm Hg. A systolic BP target <130 mm Hg may be considered in the presence of nephropathy with overt proteinuria.
Type 2 diabetes and heart failure (HF) often co-exist. Pharmacologic management of HF should include a RAAS blocker, β-blocker, and a mineralocorticoid receptor antagonist, with consideration given to supplementing these therapies with a diuretic and ivabradine.
CARDIAC PACING AND CARDIAC RESYNCHRONIZATION THERAPY
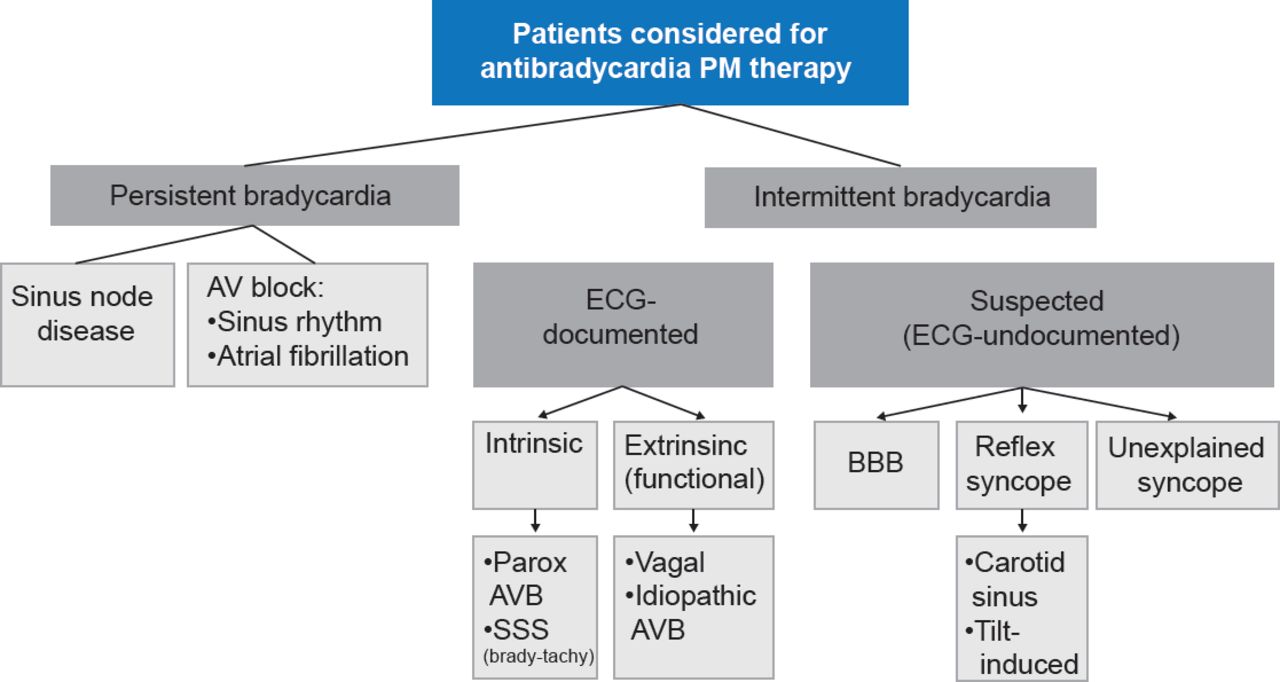
Michele Brignole, MD, Ospedali del Tigullio, Italy, delivered highlights of the 2013 ESC guidelines on cardiac pacing and CRT developed in collaboration with the European Heart Rhythm Association [Brignole M et al. Eur Heart J 2013; Europace 2013]. The Task Force created a new classification system for bradyarrhythmias (Figure 1) in which the recommendations are dependent upon the patient's clinical presentation (persistent or intermittent bradyarrhythmia) and whether it has been documented with an electrocardiogram.
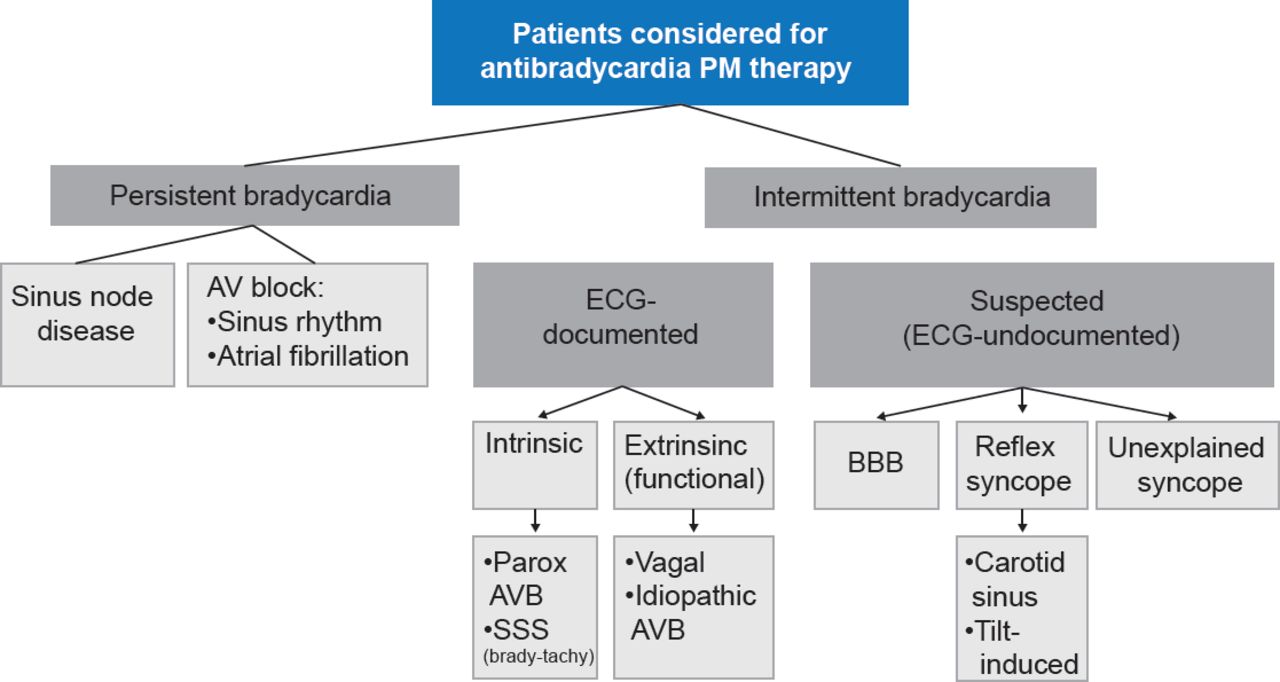
Classification of Bradyarrhythmias Based on Patient Clinical Presentation
AV=atrioventricular; AVB=atrioventricular block; BBB=bundle branch block; ECG=electrocardiogram; PM=pacemaker; SSS=sick sinus syndrome.
Reproduced from Brignole M et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology. Developed in collaboration with the European Heart Rhythm Association. Eur Heart J 2013;34(29):2281–2329. With permission from Oxford University Press.
Indications and potential for pacing according to the new guidance (Table 2):
Indications for CRT in Patients in Sinus Rhythm
-
Symptomatic sinus node dysfunction, with consideration given to pacing in the absence of conclusive evidence if symptoms are likely caused by bradycardia
-
Third-degree or type 2 second-degree atrioventricular block (AVB)
-
Consider pacing in patients aged ≥40 years with recurrent, unpredictable neurocardiogenic syncope and documented symptomatic pauses despite alternative therapies
-
Syncope with bundle branch block (BBB) and a His-ventricular interval ≥70 ms or pathologic AVB during atrial pacing
-
Alternating BBB, even if the patient is asymptomatic
ARTERIAL HYPERTENSION
The 2013 guidelines for the management of arterial hypertension were produced jointly by the ESC and European Society of Hypertension (ESH) [Mancia G et al. Eur Heart J 2013; J Hypertens 2013]. Task Force chairs Giuseppe Mancia, MD, PhD, University of Milano-Bicocca, Milan, Italy, and Robert Fagard, MD, PhD, KU Leuven University, Leuven, Belgium, presented the overview.
Out-of-office BP monitoring takes on a more important role in the new guidelines, and should be considered an adjunct to office BP recording in the diagnostic evaluation. The definition for hypertension is an office BP ≥140/≥90 mm Hg or a daytime ambulatory/home BP of ≥135/≥85 mm Hg. One specific indication for ambulatory BP monitoring is a marked discordance between office BP and home BP.
The guidance indicated no treatment for patients with high normal BP (130 to 139/85 to 89 mm Hg). A major development was the decision to recommend a single systolic BP target of 140 mm Hg for almost all patients, reversing the separate targets for moderate- to low-risk patients (140/90 mm Hg) and high-risk patients (130/80 mm Hg) in the 2007 version of the guidelines.
A greater emphasis on assessing total CV risk is contained in the 2013 guidelines (Table 3). Additional risk factors such as organ damage, diabetes, and other CV risk factors need to be considered before initiating treatment and during follow-up. For patients aged ≥65 years, there is solid evidence to recommend reducing systolic BP to 150 to 140 mm Hg, said Prof. Fagard.
Total Cardiovascular Risk Stratification
There is no specific preference for single-drug therapy, and an updated protocol for drugs taken in combination. The beneficial effect of hypertension depends largely on BP lowering rather than the choice of drug, so no hierarchy of drugs is suggested.

The editors would like to thank the many members of the European Society of Cardiology presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.