

Summary
Americans need to eat healthier, but dietary guidelines and model dietary patterns are not enough to ensure that they do so. This article reviews the evolution of the Dietary Guidelines for Americans (DGAs).
- Nutrition Physiology
- Nutrition Guidelines
- Nutrition Physiology
- Nutrition
- Nutrition Guidelines
Americans need to eat healthier, but dietary guidelines and model dietary patterns are not enough to ensure that they do so. Johanna Dwyer, DSc, RD, a contractor at the Office of Dietary Supplements, National Institutes of Health, Bethesda, Maryland, USA, reviewed the evolution of the Dietary Guidelines for Americans (DGAs).
Starting in 1980, new DGAs have been issued every 5 years [http://www.cnpp.usda.gov/DGAs1980Guidelines.htm]. In 1980, the United States Departments of Agriculture (USDA) and Health, Education and Welfare (now the Department of Health and Human Services [HHS]) issued Nutrition and Your Health: Dietary Guidelines for Americans [USDA/HHS 1980], a 20-page brochure that offered seven recommendations (Table 1). The early guidelines recommended increased complex carbohydrate consumption and reductions in fat (particularly saturated fat), cholesterol, sugar and salt consumption, and moderation in alcohol if it was consumed at all.
Recommendations From the 1980 DGAs on Nutrition and Health
As each subsequent DGA was issued, the paradigm shifted. Importantly, there has been a gradual shift from recommendations based on expert opinion alone to guidance developed after more formal and systematic review and synthesis of the evidence followed by expert reviews and judgments based on it. There has also been increasing transparency in the guideline development process: committee meetings are open and the evidence library is now publically available. Public comments are accepted throughout the process including the advisory committee reports, the report is reviewed by agencies, and agency authored policy documents. Fundamental changes in the guidelines themselves include a shift away from a focus on a core pattern to ensure adequacy such as the basic 4 food groups (fruits, grains, vegetables, and protein) to a total dietary intake approach to include concerns about adequacy, balance and moderation, from dietary intake alone to energy balance both intake and output, and emphasis on lifestyle, and a shift from concerns about getting an adequate diet to worries about excess food consumption. The more recent guidelines include people at risk (instead of just healthy people). They also provide suggestions on what individuals should do to have a healthier diet, not just the things to avoid. By 2020 future guidelines may also be available for children under the age of 2.
The DGAs have had a positive effect on the risk factors associated with a poor diet. For instance, randomized controlled trials and feeding studies have shown that eating plans based on the DGAs like the Dietary Approaches to Stop Hypertension (DASH) pattern and MyPlate can decrease blood pressure. Other studies have shown a link between healthy eating patterns and reduced risk of cardiovascular disease. DGAs have been used as the basis for changing federally supported school lunch and breakfast menus, meal planning and master menus for the Department of Defense, and many other programs. The DGAs are based on the Dietary Reference Intakes (DRIs) and are linked to other dietary guidance tools such as the MyPlate icon, the Nutrition Facts labels on foods, allowable health claims for foods, and nutrition recommendations used to develop diets for schools, prisons, hospitals, and nursing homes, in the development of new packaged foods, and as part of healthcare policymaking.
There have been missteps along the way in DGA development, however. Solid fat and added sugars (so-called “empty calories”), nutrient density, and discretionary calories have proven to be difficult concepts for the average consumer to comprehend, and the guidelines appear to have done little to clarify or educate on these matters. Many Americans also do not understand what makes a grain a “whole grain” or the impact of alcohol on obesity.
To improve the DGAs, Dr. Dwyer suggests broadening the background of those scientists involved in their development to include experts in the areas of dietetics, food science, food safety, food waste, and food production. The communication of resulting guidelines needs to involve other experts, such as those in social science, behavioral science economics and ecology. She recommends that the Dietary Guidelines Advisory Committee (DGAC) continue to use and strengthen systematic evidence-based reviews to assess the state of the science for the effects of nutrition and food safety on health, and provide advice on dietary guidelines for the general public based on preponderance of current scientific and medical information. The focus should be on ultimate nutritional and health results, and not solely on the process or technology it takes to get there. Other recommendations for improvement include developing specific recommendations for individuals with different lifestyles, different foods budgets, and for different ethnic groups so that they can better apply the DGAs. As time goes on and work to identify genetic predispositions for chronic conditions whose risks can be reduced by appropriate diets progresses, we may reach the point where it is possible to provide individually tailored dietary recommendations as well. Finally there needs to be an update to the Healthy Eating Index to permit quick assessment of diet quality after the 2015 Guidelines are issued.
Dr. Dwyer stated that ensuring food for all human beings is both an ethical issue and a moral imperative, but eating according to the DGAs is a health issue, not a moral issue. Good science should lead to politics, policy, and advocacy, and not the reverse. Using the DGAs to advocate for other political agendas is unhelpful and weakens support for the overall effort. Dr. Dwyer cautions against mission overreach, making definitive pronouncements on poorly understood science and technology. There is always the danger of wandering into peripheral areas beyond the committee's core expertise while neglecting to focus on the committee's fundamental charge. There are risks from ignoring unintended consequences such as failure to consider food preparation time and costs. Finally, Americans must learn from the past that implementation is difficult. The DGAs alone cannot change consumption patterns. Paradigms change but there remains a need for partnership in solving problems. Changing America's eating habits will require a team effort on the part of policy makers, government, nutritionists, dietitians, food scientists, the food industry, educators, marketers, and communicators
DRI is a collective term that includes several nutrient-based dietary reference values: estimated average requirements, recommended dietary allowances, adequate intake, and tolerable upper intake levels. Together with systematic evidence-based reviews of diet and health, DRIs form the basis of the DGAC Report that sets policy and the standards for the DGAs that guide all of the federal food programs. The DRIs are set by the Food and Nutrition Board (FNB) and the Institute of Medicine and are used by both the United States and Canada.
Suzanne P. Murphy, PhD, RD, University of Hawaii, Honolulu, Hawaii, USA, discussed the need to update the DRIs. Her recommendations include the use of a core FNB committee that would focus on updating and extending nutrient standards. This would reduce costs, while allowing the FNB to continue the task of setting nutrient standards. DRI and DGA updates should be conducted every 10 years.
Dr. Murphy reviewed the latest edition of the Dietary Guidelines for Americans, 7th Edition [USDA/HHS. Washington, DC: US Government Printing Office, December 2010]. Although divided into chapters that focus on particular aspects of eating patterns, the 2010 guidelines provide integrated recommendations for health. To get the full benefit, individuals are encouraged to carry out these recommendations in their entirety as part of an overall healthy lifestyle.
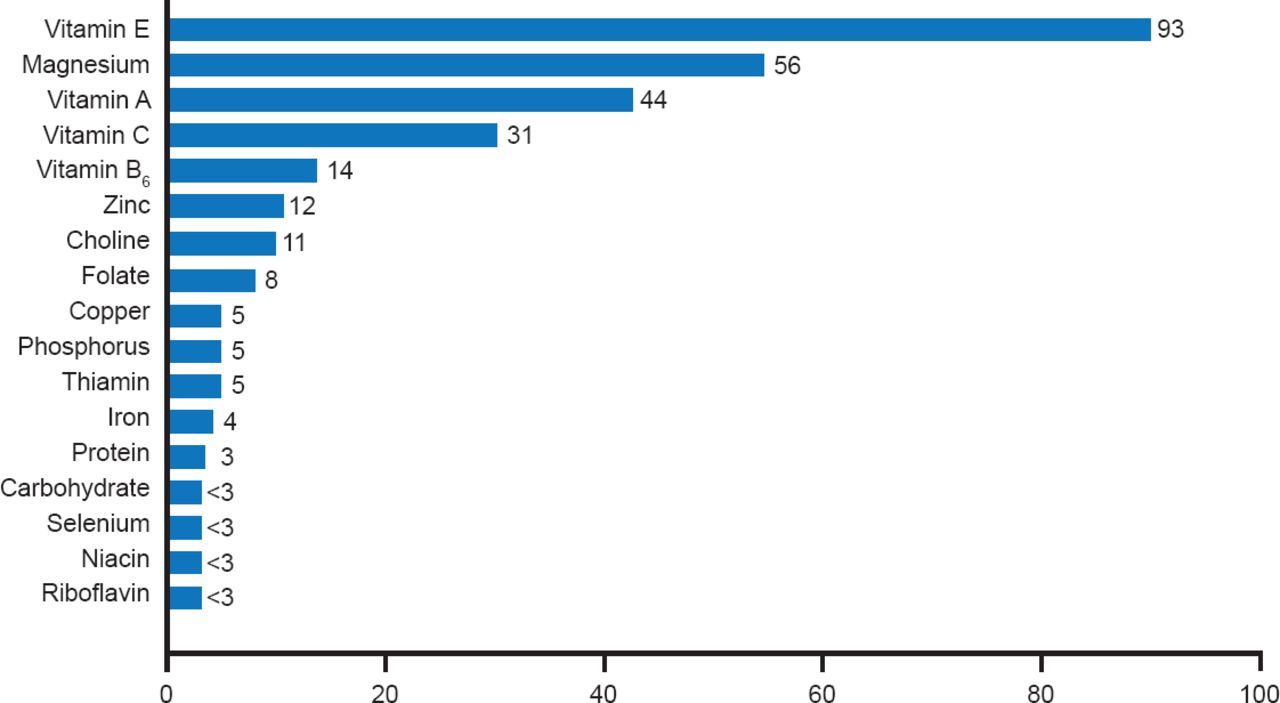
Chapter 1 introduced the concept of nutrient density and reported on the evaluation of nutrient intakes of Americans, which was inadequate in certain nutrients such as vitamin A, E, and C as well as magnesium according to a National Health and Nutrition Examination Survey (Figure 1) [USDA, Agricultural Research Service. What We Eat in America, NHANES 2001–2002. September 2005].

Percentage of Americans With Inadequate Nutrient Intakes
Source: Moshfegh A et al. What We Eat in America. NHANES 2001–2002: Usual Nutrient Intakes from Food Compared to Dietary Reference Intakes. U.S. Department of Agriculture, Agricultural Research Service 2005.
Chapter 2 discussed how to use estimated energy requirements to balance energy intake with physical activity and manage weight. Foods and food components to reduce caloric imbalances were covered in Chapter 3, while Chapter 4 discussed how to increase foods that provide more potassium, dietary fiber, calcium, vitamin D, and seafood (omega-3 fatty acids). Chapter 5 outlined healthy eating patterns that met all DRIs without exceeding energy DRIs and upper intake levels. Dietary guideline recommendations for 12 vitamins, 9 minerals, and 8 macronutrients with separate nutrient goals for each age/sex group based on their needs were also included [USDA/HHS. Dietary Guidelines for Americans, 7th Edition, Washington, DC: US Government Printing Office, December 2010]. Ultimately, the food patterns reported led to consumer guidance for a nutritionally adequate diet called “MyPlate” (Figure 2).

Chapter 6 discussed how DRIs inform nutrition fact labels, nutrition education programs, food assistance programs, and help Americans make healthy food choices.
Although DRIs have been set for many nutrients, most have not been reviewed recently and are in need of updating and revision. However, no reviews by the FNB are currently in process, government funding is lacking, and there is no consensus regarding how to move forward. A brochure is in progress on the importance of DRIs that will help to emphasize that current DRIs are key to nutrition monitoring and the development of many types of nutrition guidance and programs.
Meanwhile a core FNB committee is being considered that would be convened to ensure a periodic review of all DRI values and interface with the proposed government nomination process for major updates with the goal to insure that DRI values remain current. A review of the DGAs for each nutrient is being considered that consists of an appropriate analytic framework, a literature search using relevant key words, reviews of abstracts and papers, consultation with nutrient experts, and consensus building.
An experimental literature review showed that an appropriately thorough search was not a trivial task and indicated the types of expertise that will be needed on a core review committee. A division of expertise to complete this task is recommended. The DRI core committee should focus on updating and extending nutrient standards. The DGAC should focus on applying these standards to food choices and dietary patterns. Dr. Murphy urged those in the audience to get more involved in the process.
Grains are low in lysine and legumes are low in methionine and many cultures have grains as the base of the diet, including bread, rice, pasta, or tortillas. Whole grains are good sources of B vitamins, iron, calcium, magnesium, phosphorus, and fiber. They have been included in the DGAs for some time, but most Americans do not consume enough of them. In part this is because of a poor job that has been done in educating the public about what whole grains are and how consumers can incorporate them into a daily diet, noted Joanne Slavin, PhD, RD, University of Minnesota, St. Paul, Minnesota, USA.
There is no perfect diet. Humans are adaptable and have survived and prospered on many types of diets often based on the access to a certain food supply. For instance, in the traditional Arctic diet, 80% of kcals are obtained from fat while 80% of kcals are obtained from carbohydrates in the traditional African diet [Slavin J. Nutrition Bulletin 2012]. At only 15 g/day, compared with the recommended intake of 25 to 38 g/day (≥3 servings), the American diet is particularly deficient in dietary fiber [Slavin JL. J Am Diet Assoc 2008]. White flour and white potatoes provide the most fiber in the US diet. We need to add functional fiber to foods to reach the recommended dietary fiber goals.
Whole grains consist of an outer shell or bran that protects the seed, the germ, which provides nourishment for seed, and the endosperm that provides energy. Each layer contains unique combinations of nutrients. To be considered a whole grain, a product must be made from the whole kernel or contain relative proportions of the three parts. Milling removes the bran and germ layers and reduces vitamin, mineral, phenolic, and fiber content. However, texture, flavor, appearance, and shelf life are improved.
Whole grains gained importance when a connection was made between high whole grain intake and lower rates of coronary heart disease, serum cholesterol, and type 2 diabetes. A connection was also made with obesity. In one study, weight gain was inversely associated with the intake of high-fiber, whole-grain foods but positively related to the intake of refined-grain foods [Liu S et al. Am J Clin Nutr 2003].
Despite lack of strong evidence, most guidelines recommend increase consumption of whole grains and reduced consumption of refined grains (Figure 3).

Whole Grains Dietary Guidance
Reproduced wth permission from J Slavin, PhD, RD.
In another study, researchers reported that consumption of foods rich in cereal or mixtures of whole grains, and bran is modestly associated with a reduced risk of obesity, type 2 diabetes, and cardiovascular disease [Cho SS et al. Am J Clin Nutr 2013].
The data for whole grains are limited primarily because of varying definitions among epidemiologic studies concerning what, and how much, was included in that food category. One meta-analysis found that whole grain intake did not affect body weight, but there was a small effect on percentage of body fat [Poi K et al. Am J Clin Nutr 2013]. Although epidemiologic studies found an association between diets high in whole grains and lower C-reactive protein (CRP) concentrations, interventional studies saw no effect of whole grain intake on CRP or other markers of inflammation [Lefevre M, Jonnalagadda S. Nutr Rev 2012]. Thus, controversy concerning the benefits of whole grains continues.
Part of the problem is that different foods contain different amounts of whole grain. The US Food and Drug Administration will approve a whole grain health claim only when at least 51% of product weight is whole grain and when the product is low in total fat, saturated fat, and cholesterol. The government puts its stamp of approval on three levels of whole grains (Figure 4).

There has been no universal standard to define what constitutes a “whole grain food” creating challenges for researchers, the food industry, regulatory authorities, and consumers. In May 2013, the American Association of Cereal Chemists International recommended that whole grain food products contain at least eight grains or more of whole grain per 30 g serving.
Although historically nutritionists have supported whole grains as a source of fiber, stricter dietary rules are difficult to support with evidence-based nutrition science. Americans need to replace some refined grains with whole grains, not eat more whole grains. In the future, solving important nutrition problems will require partnerships based on trust among academics, the government, commodity groups, activists, and food companies.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.