

Summary
It is currently estimated that 5.1 million adults in the United States have heart failure (HF). By the year 2030, this number is expected to increase by 25%. Over the last several decades, there has also been a marked increase in the prevalence of diabetes [Centers for Disease Control and Prevention. Available at http://www.cdc.gov/diabetes/statistics]. This article discusses the relationship between and coexistence of these two diseases including whether the presence of diabetes should influence the management of patients with HF, and diabetic cardiac dysfunction—lipotoxic cardiomyopathy.
- Heart Failure
- Diabetes & Endocrinology Clinical Trials
- Heart Failure
- Diabetes & Endocrinology Clinical Trials
- Cardiology
It is currently estimated that 5.1 million adults in the United States have heart failure (HF). By the year 2030, this number is expected to increase by 25%. Over the last several decades, there has also been a marked increase in the prevalence of diabetes [Centers for Disease Control and Prevention. Available at http://www.cdc.gov/diabetes/statistics]. David Aguilar, MD, Baylor College of Medicine, Houston, Texas, USA, discussed the relationship between and coexistence of these two diseases.
Diabetes has long been known to amplify the risk for all forms of cardiovascular disease (CVD) and when it develops in patients with HF, it is associated with increased mortality (Table 1) [Cubbon RM et al. Diab Vasc Dis Res 2013; Martinez-Selles M et al. Eur J Heart Fail 2012; MacDonald MR et al. Eur Heart J 2008; From AM et al. Am J Med 2006].
Increased Mortality in Patients With HF and Diabetes Mellitus
The increased mortality is even more striking among older individuals (aged ≥65 years) with diabetes who go on to develop HF, with such patients having a mortality rate of 32.7/100 person-years compared with similarly aged diabetes patients without HF who have a mortality rate of 3.7/100 person-years (HR, 10.6; 95% CI, 10.4 to 10.9) [Bertoni AG et al. Diabetes Care 2004]. The coexistence of diabetes and HF is also associated with an increased the rate of HF hospitalizations [Shah AM et al. Eur J Heart Fail 2010; MacDonald MR et al. Eur Heart J 2008; Murcia AM et al. Arch Intern Med 2004]. Future studies are needed to better understand the complex interaction of these 2 diseases and to develop treatment strategies to lower the health burden of HF and diabetes, noted Dr. Aguilar.
Mary N. Walsh, MD, St. Vincent Heart Center, Indianapolis, Indiana, USA, discussed whether the presence of diabetes should influence the management of patients with HF. Dr. Walsh reinforced diabetes as a driver of HF adding that this is particularly true for women [Levy D et al. JAMA 1996], even among those with no other risk factors and especially when the diabetes is uncontrolled [Bibbins-Domingo K et al. Circulation 2004]. She then asked “Are diabetic patients HF patients?” The answer is “Yes” according to the 2001 American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) guidelines for the evaluation and management of chronic HF in adults [Hunt SA et al. J Am Coll Cardiol 2001] in which Stage A HF includes patients with diabetes.
Whether and how diabetes influences short- and long-term outcomes among patients with HF appears to be related to multiple factors including time, age, and sex. In one study of >116,000 patients (13% with diabetes), diabetes was a significant independent predictor of mortality at 1 year. The longer term risk was greatest in younger patients, particularly women. Diabetes was also a significant independent predictor of readmission for HF, and again, the risk was greatest in younger women [MacDonald M et al. Circ Heart Fail 2008].
The 2013 ACCF/AHA guideline for the management of HF provides some guidance for how to treat patients with diabetes and HF [Yancy CW et al. J Am Coll Cardiol 2013]. Among patients with Stage A HF, the 2013 guidelines recommend that clinicians make every effort to control hyperglycemia (Class I, Level of Evidence [LoE] C), even though control has not yet been shown to reduce the subsequent risk of HF. The reason for this is that many of the standard diabetes therapies can prevent the development of other HF risk factors and may by themselves directly lower the likelihood of HF. The guidelines recommend angiotensin-converting-enzyme (ACE) inhibitors (or angiotensin II receptor blockers [ARBs] in patients intolerant of ACE inhibitors) for all patients (regardless of diabetes status) with Stage C HF with reduced ejection fraction (HFrEF) and current or prior symptoms (both Class I, LoE A). With respect to β-blockers, the current guidelines recommend the use of bisoprolol, carvedilol, or sustained-release metoprolol succinate for all patients with current or prior symptoms of HFrEF (Class I, LoE A). In HF patients with diabetes, the marked clinical benefits of these therapies are considered to outweigh the risks of hypoglycemia and dyslipidemia or decreased insulin sensitivity. Clear benefit has also been shown for aldosterone receptor antagonists in HF patients with a history of diabetes (Class I, LoE B). Patients with diabetes, left ventricular dysfunction, mildly symptomatic HF, and wide QRS complex derive similar benefit from cardiac resynchronization therapy defibrillation compared with patients without diabetes [Martin D et al. Circ Heart Fail 2011], and those without significant diabetic complications are eligible for transplantation [Russo M et al. Circulation 2006]. There are no differences in the recommendations for patients with diabetes and HF with preserved ejection fraction.
Daniel Kelly, MD, Sanford-Burnham Medical Research Institute at Lake Nona, Orlando, Florida, USA, discussed an emerging theory in diabetic cardiac dysfunction-lipotoxic cardiomyopathy, which he believes reflects a more systemic problem driven by caloric excess.
For centuries, pathologists have noted an accumulation of neutral lipids in cardiac myocytes during autopsy of morbidly obese individuals, many of whom had diabetes. More recently imaging studies in living patients with obesity and diabetes have shown evidence of increased myocardial fatty acid utilization and cardiac steatosis [Herrero P et al. J Am Coll Cardiol 2006; Szczepaniak LS et al. Magn Reson Med 2003]. These results, along with other studies focused on glucose toxicity and microvascular disease have led to a general view of the metabolic disturbances that occur in diabetic cardiac dysfunction. This view begins with insulin resistance in type 2 diabetes that reduces the ability of the heart to use glucose as fuel and consequently forces increased fatty acid burning, which in turn results in lipid accumulation that is associated with early-stage diastolic and then systolic ventricular dysfunction, and sensitivity to ischemic insult. The rationale for serum lipid-lowering strategies in the treatment of diabetic cardiomyopathy has been demonstrated in several preclinical mouse models [Duncan JG et al. Circulation 2010; Yang J et al. Circ Res 2007; Finck BN et al. Proc Natl Acad Sci USA 2003].
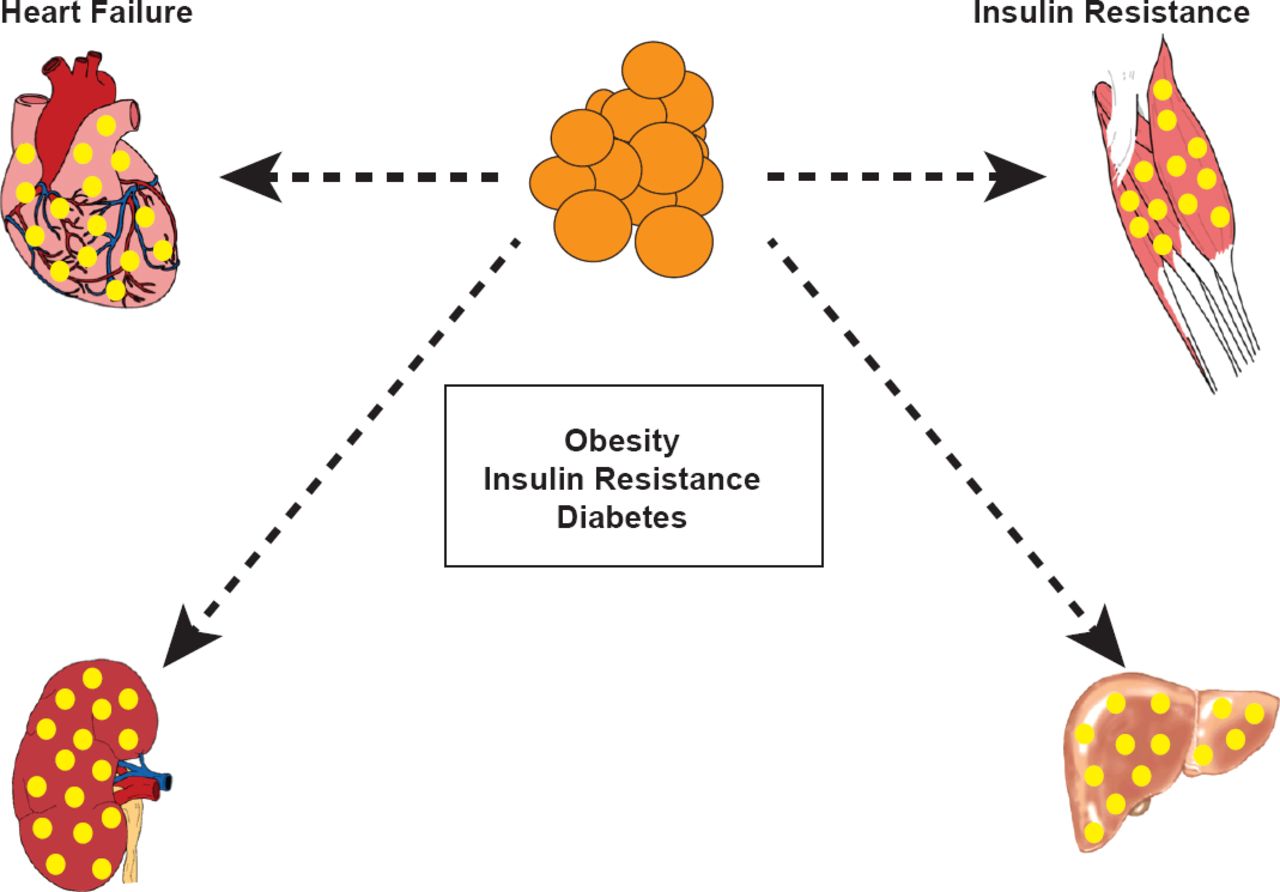
Dr. Kelly presented a model for lipotoxic organ dysfunction (Figure 1) in which the adipocytes have no more capacity to store fat and the calories end up in other tissues as neutral lipid droplets—including the heart. To define the mechanism and perhaps identify targets for metabolic modulator therapy that would be given along with traditional HF therapy, Dr. Kelly and colleagues have embarked on a small-molecule high throughput screen. One promising compound has been shown to reduce myocyte triglyceride accumulation and increases fat burning capacity, fatty acid oxidation rates, and glucose uptake. Further studies are needed to determine if this compound has the potential improve clinical outcomes in patients with diabetes and warrents further study.

Systemic Model of Lipotoxic Organ Dysfunction
Reproduced with permission from D Kelly, MD.
Although the exact mechanism remains unclear there is little doubt that there is a relationship between diabetes and HF and that the incidence of both of these life altering diseases is increasing. Patients with diabetes should be encouraged manage their risk through lifestyle changes and adherence to their treatment regimen. Clinicians treating patients with HF should manage their patients according to published guidelines.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.