

Summary
The frequency of sudden cardiac arrest (SCA) is inversely related to left ventricular function; yet, many events occur in patients with ejection fraction >35% who are not candidates for an implanted cardioverter defibrillator. The aim of the Prediction of Arrhythmic Events with Positron Emission Tomography study [PAREPET] [Fallavollita JA et al. Contemp Clin Trials 2006] was to determine if the risk of SCA in medically treated patients with Class I—III heart failure can be predicted by the volume of denervated, hibernating, or infarcted myocardium.
- Interventional Techniques & Devices
- Prevention & Screening Clinical Trials
- Cardiac Imaging Techniques
- Imaging Modalities
- Radiography
- Heart Failure
The frequency of sudden cardiac arrest (SCA) is inversely related to left ventricular (LV) function; yet, many events occur in patients with ejection fraction (EF) >35% who are not candidates for an implanted cardioverter defibrillator (ICD). The aim of the Prediction of Arrhythmic Events with Positron Emission Tomography study [PAREPET] [Fallavollita JA et al. Contemp Clin Trials 2006] was to determine if the risk of SCA in medically treated patients with Class I–III heart failure (HF) can be predicted by the volume of denervated, hibernating, or infarcted myocardium. James A. Fallavollita, MD, University of Buffalo, Buffalo, New York, USA, presented recent findings.
A total of 204 patients with coronary artery disease (CAD) who were eligible for an ICD for the primary prevention of SCA were enrolled and evaluated with positron emission tomography (PET), transthoracic echocardiography, and telephone follow-up every 3 months. At baseline, patients with prior SCA (n=33) had a mean age of 66±8 years, New York Heart Association (NYHA) functional class of 2.3±0.6, and LVEF of 25%±9%. Patients without prior SCA (n=171) had a mean age of 67±12 years, NYHA functional class of 2.1±0.8, and an EF of 28%±9%. The primary endpoint was SCA (arrhythmic death or ICD discharge for ventricular fibrillation or ventricular tachycardia >240 beats per minute). The secondary endpoint was total cardiac mortality.
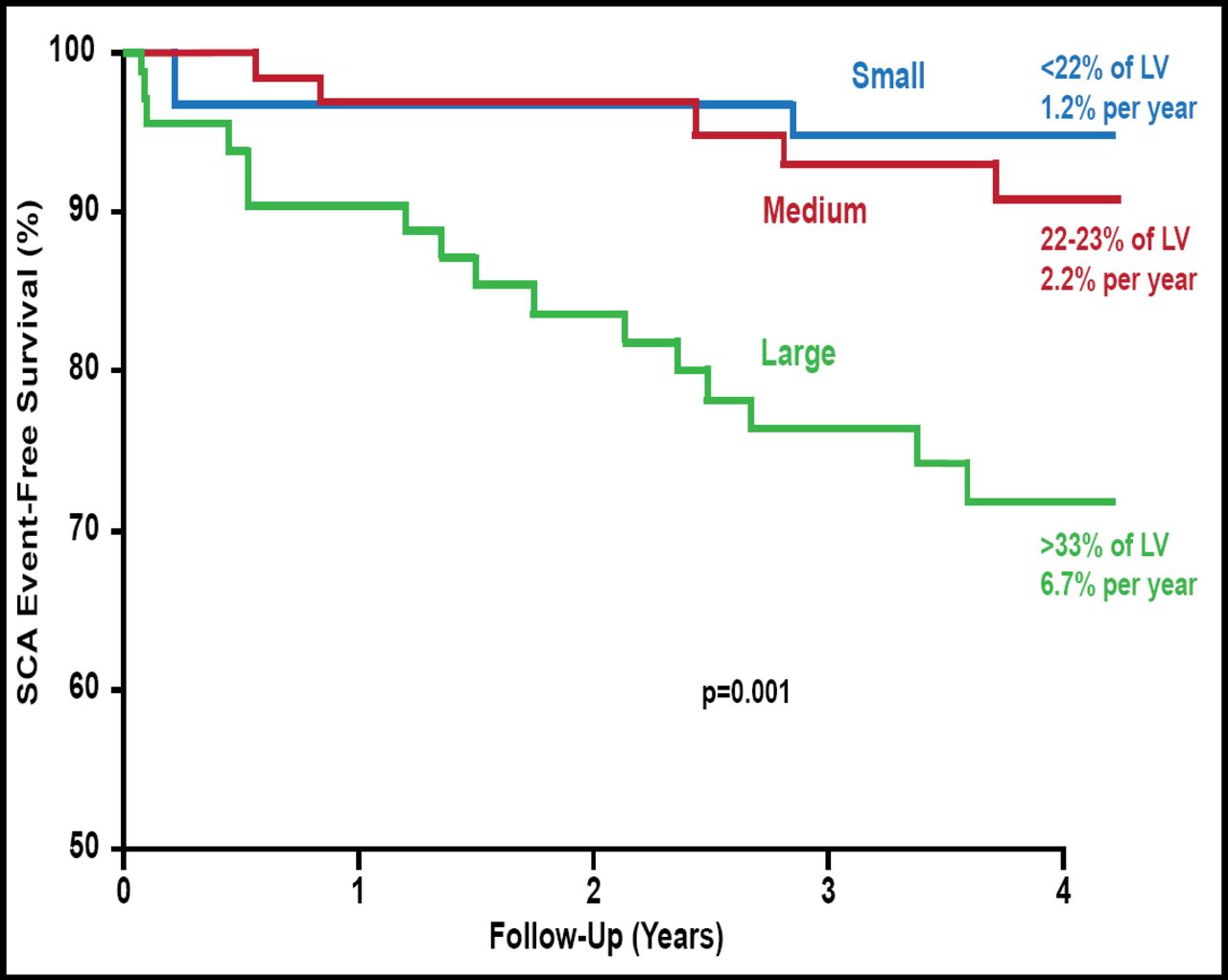
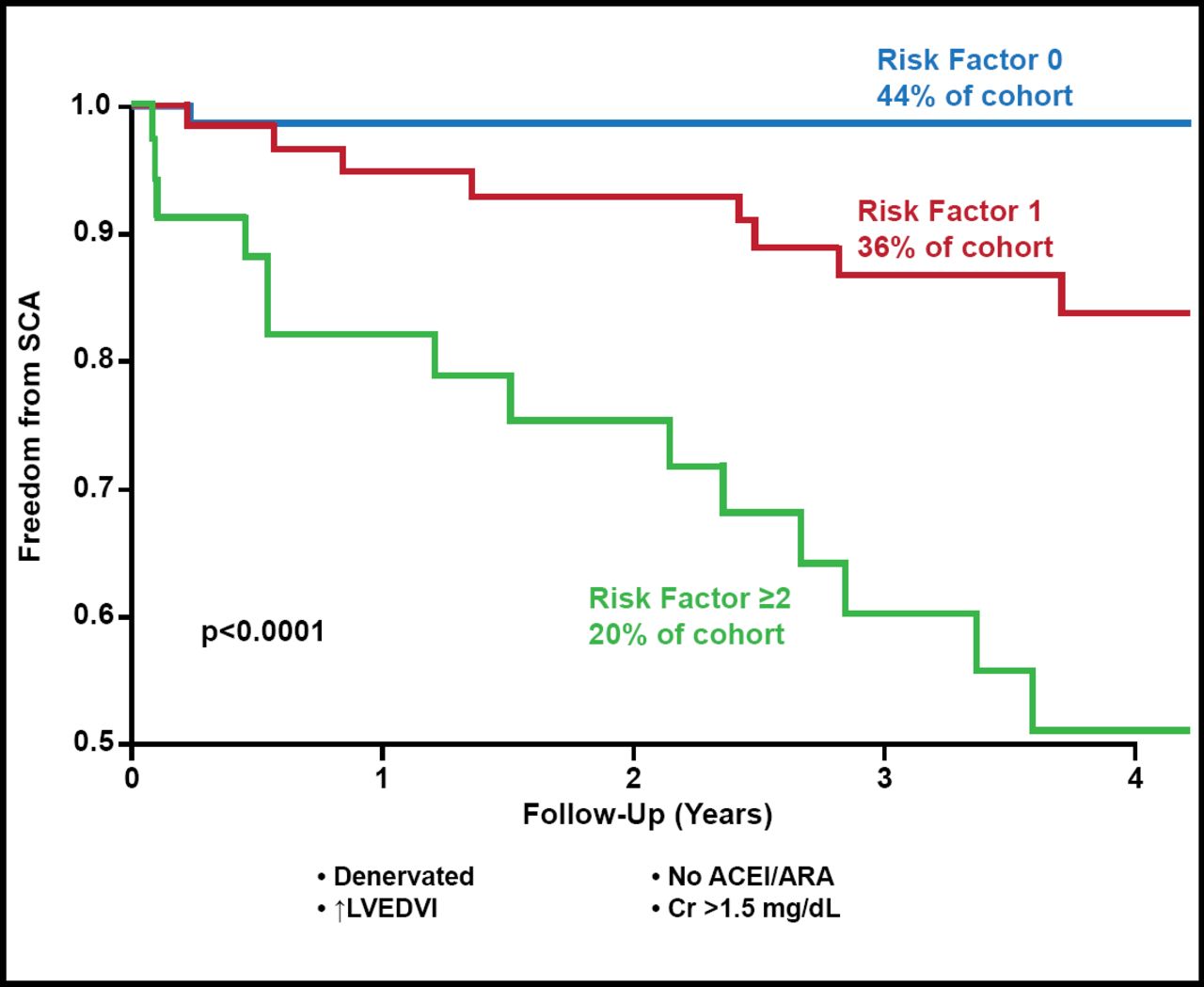
Patients with >33% denervated LV myocardium had a significantly higher rate of subsequent SCA events (6.7% per year) compared with patients with 22% to 23% denervated myocardium (2.2% per year) and <22% denervated myocardium (1.2% per year; p=0.001; Figure 1). As continuous variables, there was no correlation between the volume of infarcted or hibernating myocardium and SCA event-free survival. Multivariate analysis showed that >38% denervated LV myocardium was an independent predictor of SCA (HR, 3.5; p=0.009). Other independent predictors of SCA were LV end-diastolic volume index >98 mL/m2 (HR, 5.7; p<0.001), no angiotensin-converting enzyme inhibitor or aldosterone receptor antagonist therapy (HR, 6.8; p=0.003), and creatinine >1.5 mg/dL (HR, 3.1; p=0.005). The risk for SCA progressively increased with the number of risk factors (p<0.0001; Figure 2) and was ∼12% per year among the 20% of the cohort with 2 or more risk factors. Perhaps more importantly, the 44% of the cohort with none of the risk factors had a very low risk of SCA, averaging <1% per year.

PET Parameters and SCA.
LV=left ventricular; PET=positron emission tomography; SCA=sudden cardiac arrest.
Reproduced with permission from JA Fallavollita, MD.

Independent High-Risk Predictors of SCA.
ACEI=angiotensin-converting enzyme inhibitor; ARA=angiotensin receptor antagonists; LVEDVI=left ventricular end-diastolic volume index.
Reproduced with permission from JA Fallavollita, MD.
In patients with ischemic cardiomyopathy who are eligible for an ICD, the volume of denervated myocardium predicts SCA, independent of brain natriuretic peptide, EF, and NYHA class. The volume of infarcted and hibernating myocardium did not predict SCA. Quantitative assessment of denervated myocardium may facilitate more effective targeting of ICDs for primary prevention. Furthermore, the quantification of denervated myocardium has the potential to identify an increased risk of SCA among individuals with more preserved LVEF who are not currently considered candidates for an ICD.
- © 2012 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.