

Summary
This article discusses the impact and management of tricuspid valve disease. Although much attention in clinical practice and research on patients with valvular heart disease has focused on disorders of the mitral and aortic valves, tricuspid regurgitation can also be associated with significant morbidity and mortality.
- Valvular Disease
Edward B. Savage, MD, Cleveland Clinic Florida, Weston, Florida, USA, discussed the impact and management of tricuspid valve (TV) disease. Although much attention in clinical practice and research on patients with valvular heart disease has focused on disorders of the mitral and aortic valves, tricuspid regurgitation (TR) can also be associated with significant morbidity and mortality.
Nath et al. [J Am Coll Cardiol 2004] reported that 1-year survival in patients with no, mild, moderate, and severe TR (n=5223) was 91.7%, 90.3%, 78.9%, and 63.9%, respectively. TR severity was associated with worse survival regardless of left ventricular ejection fraction or pulmonary artery pressure.
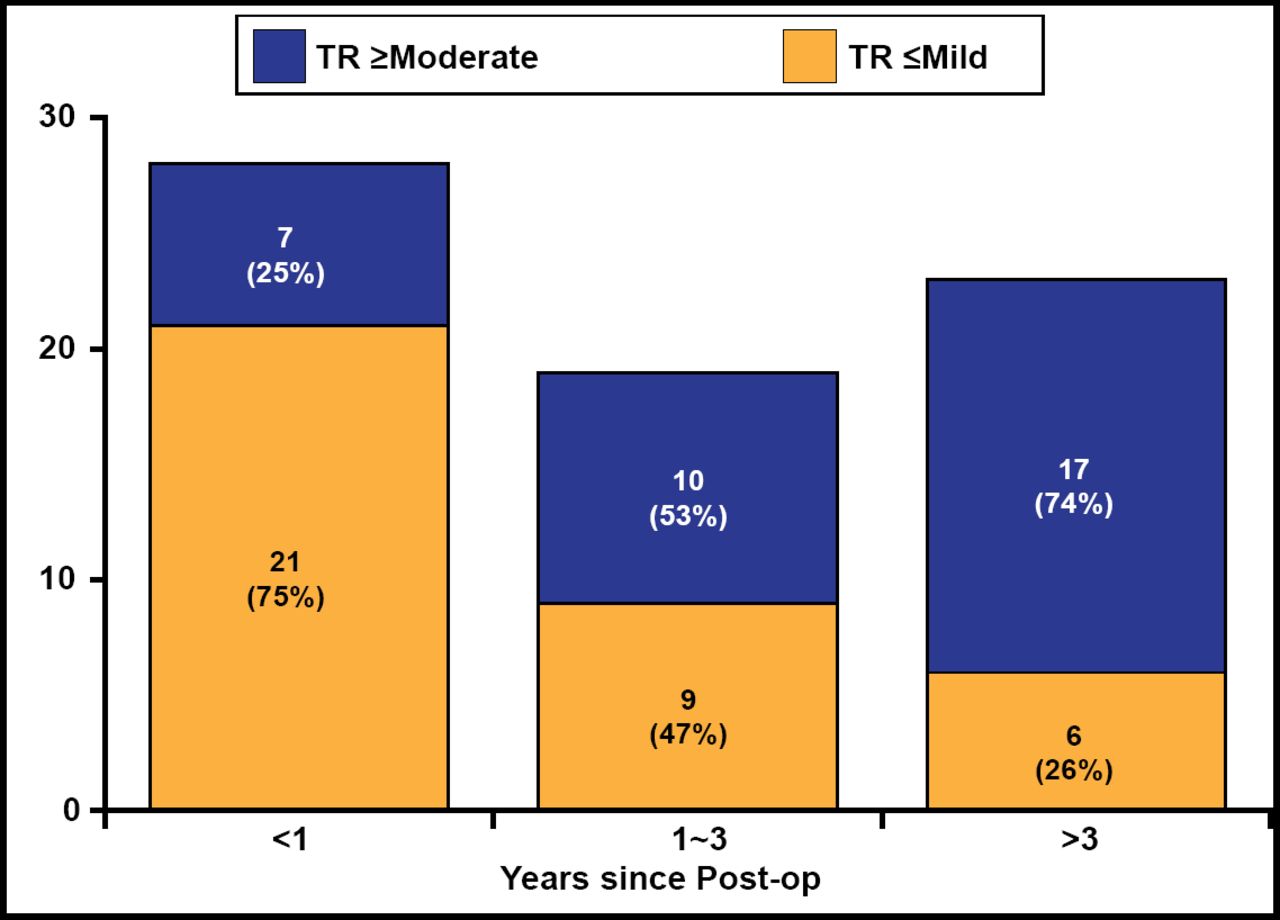
Matsunaga et al. [Circulation 2005] evaluated 70 patients with mitral regurgitation (MR) ≤1+ after repaired functional ischemic MR. Among 21 patients with preoperative TR, 4 of 9 (44%) who had TR repair and 8 of 12 (67%) without TR repair had residual postoperative TR. At <1 year, only 25% had moderate or higher TR but at >3 years, 74% had moderate or higher TR (Figure 1). Among patients with recurrent ischemic MR, 64% with moderate or higher MR and 42% with no or mild MR had moderate or higher late TR.

Progression of TR after Repaired Functional Ischemic MR.
MR=mitral regurgitation; TR=tricuspid regurgitation
Reproduced with permission from E. Savage, MD.
Among 167 patients without organic TV disease treated with mitral valve (MV) surgery who had moderate or less functional TR preoperatively, 41.9% were treated for TR and 58.1% were not treated [Shi KH et al. Heart Surg Forum 2012]. Five-year Kaplan-Meier survival was 85.3% in the treated group versus 64.7% in the no-treatment group (p=0.001).
These studies demonstrate that functional TR is progressive, moderately severe and severe TR reduces survival, and repair of left-sided valvular lesions alone may not be sufficient.
A review of 17 studies concluded that preoperative pulmonary hypertension does not predict late TR and tricuspid annular dilation probably is the most important factor for late TR [Bianchi G et al. Interact Cardiovasc Thorac Surg 2009]. The analysis suggested that patients undergoing MV surgery should have TR repair when TR is severe or, regardless of TR severity, when annular dimension is >21 mm/m2 or ≥3.5 cm by echocardiography, intraoperative tricuspid annulus diameter is >70 mm, preoperative atrial fibrillation (AF) is present, or a trans-tricuspid pacemaker lead is present.
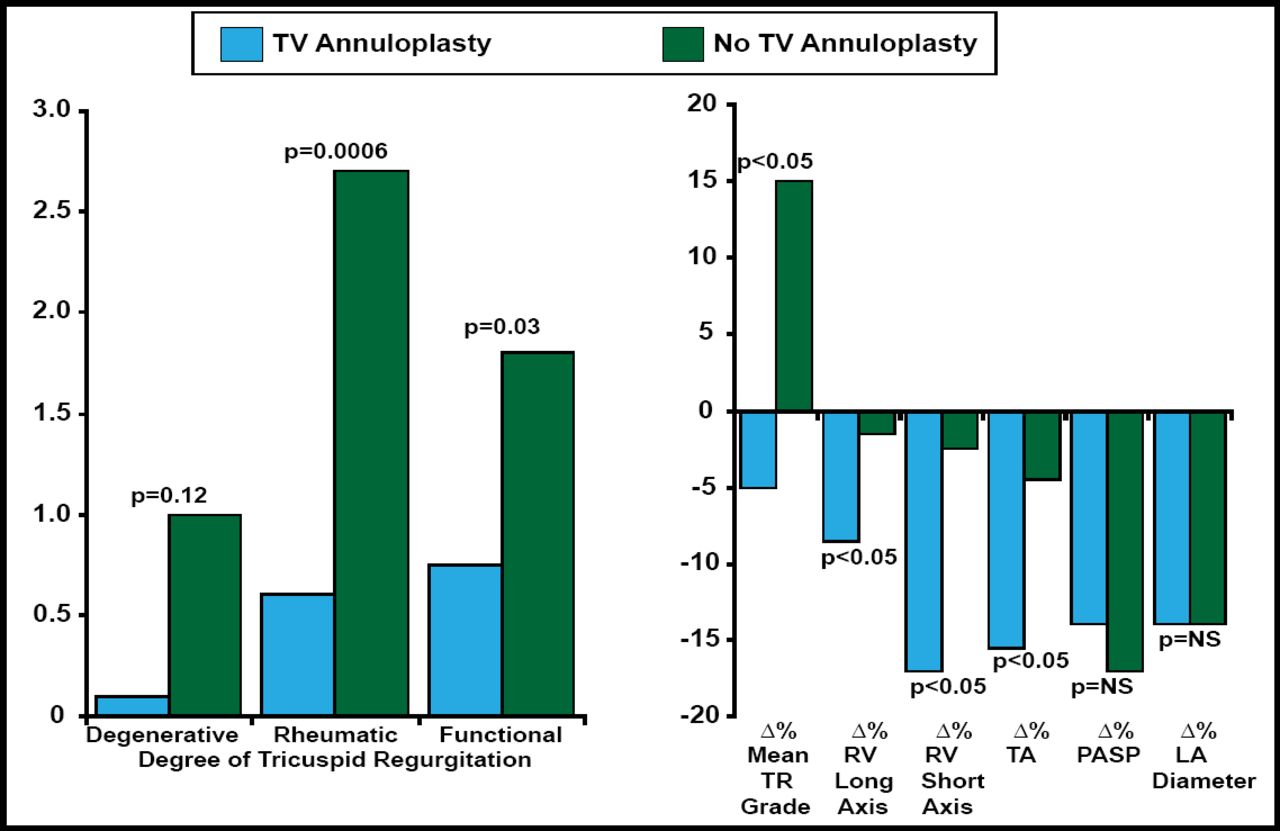
According to McCarthy and Sales et al. [Curr Treat Options Cardiovasc Med 2010], risks for TR progression after MV surgery include dilated annulus, ischemic cardiomyopathy, and pulmonary hypertension. Risks for recurrent TR after TV annuloplasty include permanent pacing wires, AF, and right ventricular dysfunction with dilation and leaflet tethering. Benedetto et al. [J Thorac Cardiovasc Surg 2012] reported that prophylactic TV annuloplasty for dilated tricuspid annulus reduced TR progression, improved right ventricular remodeling, and improved functional outcomes (Figure 2).

Prophylactic Tricuspid Annuloplasty in Patients with Dilated Tricuspid Annulus Undergoing MV Surgery.
LA=left atrial; MV=mitral valve; PASP=pulmonary artery systolic pressure; RV=right ventricular; TA=tricuspid annulus; TR=tricuspid regurgitation; TV=tricuspid valve.
Reprinted with permission from J Thorac Cardiovasc Surg 2012;143(4):844. Galbut DL et al. Bilateral internal throacic artery grafting improves long-term survival in patients with reduced ejection fraction.
Dreyfus et al. [Ann Thorac Surg 2005] performed tricuspid annuloplasty in patients undergoing MV repair if tricuspid annular diameter was greater than twice the normal size (≥70 mm). TR increased more than 2 grades in 2% of patients with tricuspid repair versus 48% of patients without tricuspid repair, demonstrating that TV annuloplasty based on tricuspid dilation improves functional status irrespective of TR grade. Chan et al. [Ann Thorac Surg 2009] found that actuarial freedom from heart failure (HF) was improved in patients who had tricuspid repair with MV replacement (5-year, 95.3%; 10-year, 92.8%) versus patients without tricuspid repair (5-year, 89.2%; 10-year, 71.2%).
Evidence shows that TR can be progressive and significantly decreases survival. TR should be treated before severe right HF symptoms develop. Tricuspid repair should be considered in patients with pulmonary hypertension, >2+ TR, or annular dilation if other heart surgery is planned.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.