

Summary
Cyanoacrylates are the main liquid adhesives used in the vascular system and have an important role in managing vascular abnormalities, especially arteriovenous malformations [Pollack JS, White RI, Jr. J Vasc Interv Radiol 2001]. This article discusses the use of glue septal ablation treatment for hypertrophic obstructive cardiomyopathy.
- Inflammatory Disease
- Cardiology
Cyanoacrylates are the main liquid adhesives used in the vascular system and have an important role in managing vascular abnormalities, especially arteriovenous malformations [Pollack JS, White RI, Jr. J Vasc Interv Radiol 2001]. Ali Oto, MD, Hacettepe University, Ankara, Turkey, discussed the use of glue septal ablation (GSA) treatment for hypertrophic obstructive cardiomyopathy (HOCM).
HOCM is characterized by asymmetric myocardial hypertrophy that is most pronounced in the interventricular septum and is responsible for the dynamic obstruction of the left ventricular outflow tract (LVOT) [Fifer MA et al. Circulation 2008]. Prof. Oto explained that LVOT obstruction is due to the hypertrophied septum and mitral regurgitation.
Alcohol septal ablation (ASA) for HOCM is a less invasive alternative to surgical myectomy to reduce the LVOT gradient in patients resistant to drug therapy [Alam M et al. Eur Heart J 2009]. A recent assessment of the technique found that a significant decrease in mean peak gradient (p<0.0001) in the LVOT was associated with a decrease in LV mass (p=0.0006) and with regression of LV hypertrophy outside the scar after ASA [Timmer SA et al. Am J Physiol 2011.
According to Prof. Oto, limitations of the ASA led him and his colleagues to publish their first-in-man GSA case in an HOCM patient with extensive collaterals to the posterior descending coronary artery that precluded alcohol ablation [Oto A et al. Catheter Cardiovasc Interv 2007].
Last year, Prof. Oto and colleagues described an approach for septal ablation with glue in HOCM patients with collateral formation to the right coronary artery in whom ASA was contraindicated [Oto A et al. J Interv Cardiol 2011]. GSA was performed in 18 patients, 6 of whom had collateral branches to the RCA. The left coronary ostium was cannulated with 6F to 8F guiding catheter. The septal branch was cannulated with a 4F catheter and microcatheter, and then cyanoacrylate mixture was instilled into the septal artery. Immediate polymerization prevented leakage into the left anterior descending (LAD) coronary artery, and also into the RCA via septal collaterals.
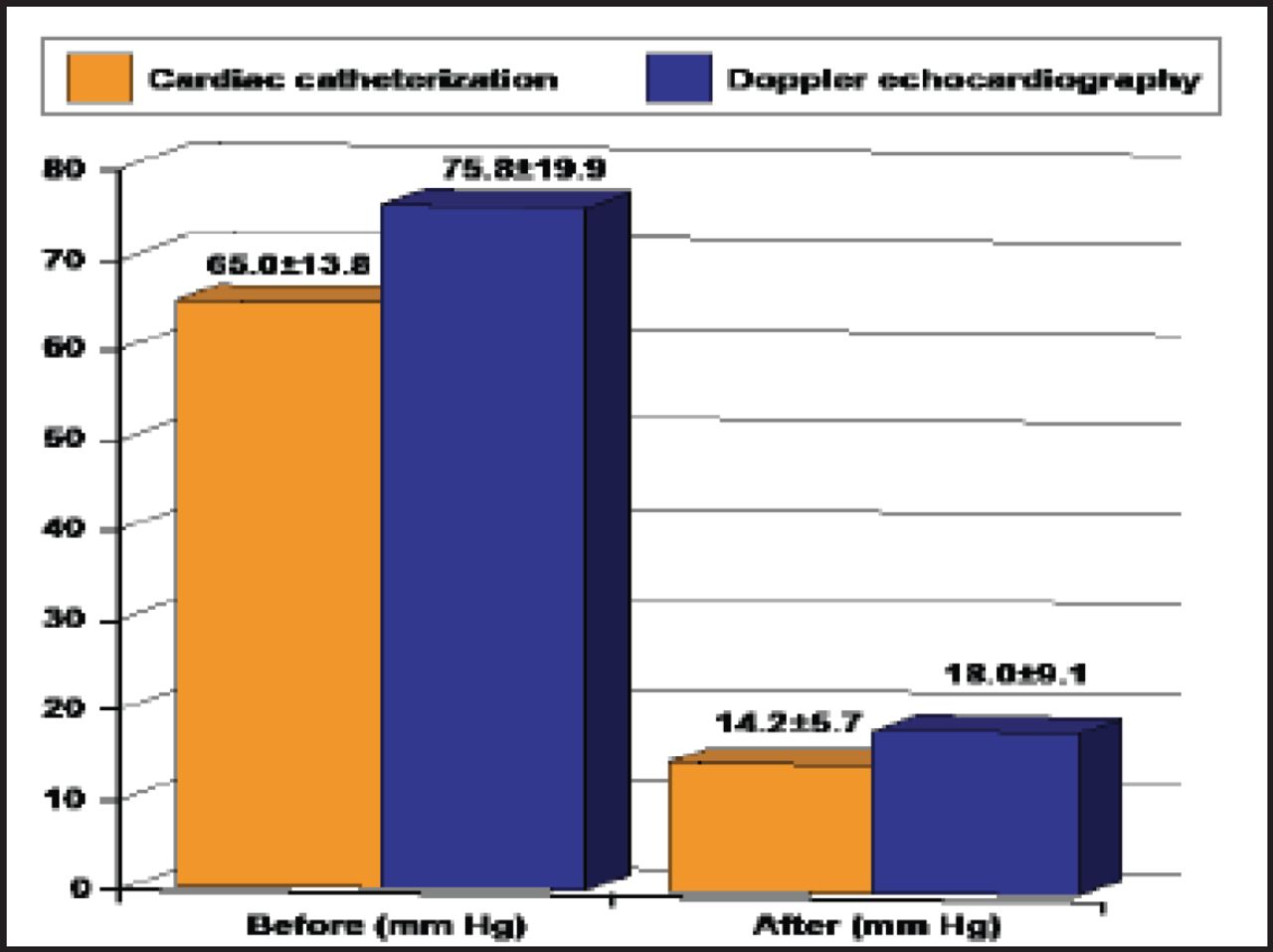
Immediately after the procedure, peak LVOT gradient reduced significantly in both cardiac catheterization (65.0±13.8 vs 14.2±5.7 mm Hg; p<0.001) and Doppler echocardiographic measurements (75.8±19.9 vs 18.0±9.1 mm Hg; p<0.001; Figure 1). Reduction in LVOT gradient persisted after 6 months of follow-up. Furthermore, septal wall thickness (20.2±3.7 vs 16.5±3.2 mm; p=0.003) significantly decreased while NYHA functional class improved (3.1±0.4 vs 2.2±0.3; p<0.001). No significant complications occurred during the procedure or within 6 months of follow-up [Oto A et al. J Interv Cardiol 2011].

Left Ventricular Outflow Tract Gradient.
Prof. Oto and colleagues concluded that GSA is a promising alternative for treating patients with HOCM. Their experience suggests that GSA is safe, effective, and can be performed without serious complications.
Glue seems to be superior to alcohol; immediate freezing prevents leakage to the LAD coronary artery and is thought to be particularly useful in the presence of collaterals. Further experience is needed to assess the long-term efficacy and safety of the technique.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.