

Summary
In an age when few new drugs are being developed, aerosol antimicrobials help old drugs work better. This article discusses the variables to consider when prescribing aerosolized antimicrobials.
- Pneumonia
- Lower Respiratory Infections
- Emerging Therapies
- Drug Resistance
In an age when few new drugs are being developed, aerosol antimicrobials help old drugs work better. David E. Geller, MD, Florida State University and University of Central Florida School of Medicine, Orlando, Florida, USA, opened the session with a discussion of the variables to consider when prescribing aerosolized antimicrobials.
An important advantage of inhaled antimicrobials is that they can directly deliver high concentrations of drug to the location of the infection while limiting systemic access and, thus, potential toxicity issues. Dr. Geller stressed that “parenteral MIC [minimum inhibitory concentration] breakpoints are meaningless in the context of inhaled antibiotics” and reminded the audience that the label dose, emitted dose, and inhaled dose are not always equal to the actual dose reaching the lungs when using aerosol delivery.
There are strategies for optimizing aerosol formulations and delivery devices, such as using very high doses, optimizing formulation (increase residence time in airways, use a higher concentration, or combinations of drugs), and optimizing delivery device (intuitive to use, shorter delivery time, reduced cleaning and disinfection time). The biggest source of deposition variability is the upper airway, so it is important for clinicians to know that because airway size changes with growth it is not necessary to adjust an aerosol dose on a mg/kg basis [Onhöj J et al. Am J Respir Crit Care Med 2000]. Controlled inspiration can also reduce variability, resulting in higher deposition [Brand P et al. J Pharm Sci 2000]. Two devices that help with inspiratory control are the I-neb and AKITA (limit inspiratory flow to 12 to 15L/min). Despite advances, inhaled treatments can be burdensome to patients and families. New technologies are being integrated to reduce that burden.
The pharmacokinetics (PK) and pharmacodynamics (PD) of aerosolized antibiotic therapy in cystic fibrosis (CF) are poorly understood. Michael Dudley, PharmD, Rempex Pharmaceuticals, San Diego, California, USA, outlined important considerations and recent progress regarding the integration of aerosol science, PK-PD, and clinical trial designs for drugs used to treat chronic and acute infections.
Overall results in clinical trials have been consistent with known PK-PD properties. It has been shown that nebulized levofloxacin produces markedly higher concentrations in sputum [Geller DE et al. Antimicrob Agents Chemother 2011] compared with what can be achieved with oral levofloxacin [Geller DE et al. North American Cystic Fibrosis Conference 2006]. Applying this knowledge in a PK model can contribute to optimized therapy by allowing the clinician to quantify drug exposure. Knowledge of a drug's PD profile also contributes to optimized treatment. For example, levofloxacin has the most rapid rate of killing among mucoid and nonmucoid isolates of Pseudomonas aeruginosa, and in contrast to tobramycin, its bactericidal activity is not affected by sputum from CF patients [King P et al. Antimicrob Agents Chemother 2010].
Population PK models incorporating both serum and lung measurements can be useful in understanding drug PK following inhalation. While differences in dosage regimen (and corresponding exposures in serum and septum) of aerosol antibiotics have been shown to result in greater overall effects, it remains difficult to link drug exposures for given patients to their clinical responses. Developing relationships between drug exposure, MICs, and clinical outcomes is difficult because of problems with intrapatient variability, while linking drug exposures to effects may be part of a larger endpoint problem in CF. MIC testing is more useful than categorical descriptions, while breakpoints are only useful following systemic administration. However, bacterial counts may be useful for designing dosage regimens.
Infection occurs early in CF and aggressive treatment with antibiotics appears to delay time to chronic infection. Current practice is to use aerosolized antibiotics in an attempt to eradicate Pseudomonas infection. Patrick A. Flume, MD, Medical University of South Carolina, Charleston, South Carolina, USA, reviewed the optimal treatment regimens for treating CF focusing on aerosol antibiotics.
An early study in patients with CF treated with aerosol tobramycin ∼600 mg 3 times/day for 12 weeks demonstrated that it was safe and effectively reduced sputum P. aeruginosa density but at the cost of increased tobramycin resistance [Smith AL et al. Pediatr Pulmonol 1989]. Hypothesizing that chronic intermittent use might overcome the problem of resistance, a later trial using a month on/month off regimen was conducted in a similar patient population with P. aeruginosa. In that study pulmonary function improved, the density of P. aeruginosa in sputum decreased, and the risk of hospitalization decreased [Ramsey BW et al. N Engl J Med 1999]. More tobramycin patients were free of exacerbation compared to placebo (p=0.014). As a result of this study use of inhaled tobramycin was added to the respiratory guidelines [Flume PA et al. Am J Respir Crit Care Med 2007].
Currently there are 2 approved aerosol antibiotics: tobramycin and aztreonam lysine inhalation. Colistmethate sodium power is approved for use in some European countries. Current research focuses on optimizing treatment regimens and whether the approach used for P. aeruginsoa will work for other pathogens.
Jean Chastre, MD, Université Pierre et Marie Curie, Paris, France, presented data supporting a rational for using aerosol drug delivery to treat ventilator-associated pneumonia (VAP). Pneumonia caused by P. aeruginosa, methicillin-resistant Staphylococcus aureus, and other multidrug-resistant organisms is associated with high morbidity and mortality despite appropriate antibacterial therapy. Relapse is frequent as pathogens are often not cleared by antibiotics.
Prof. Chrastre suggested that directly delivering antibiotics to the lung via aerosolization, as an adjunctive therapy to IV administration, may allow increased drug concentrations at the infected site. In addition, by limiting systemic exposure it could also allow the administration of antibiotics characterized by high systemic toxicity, such as polymyxins.
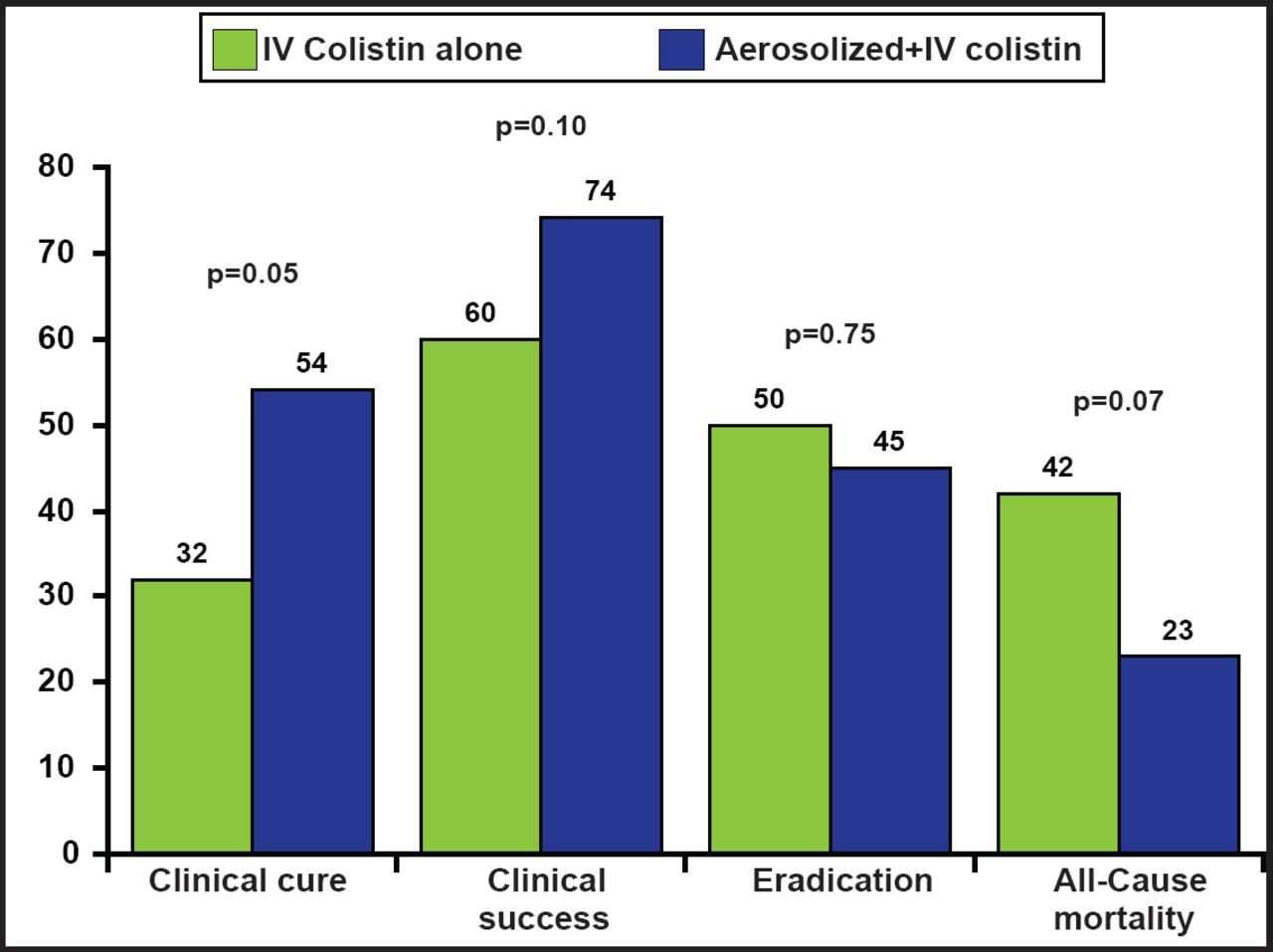
Studies suggest that compared with jet nebulizers, ultrasonic and ceramic vibrating plate devices provide higher lung tissue deposition as they generate particle size well below <10µ in diameter. In a recent study the use of adjunctive inhaled therapy significantly decreased the use of IV antibiotics [Niederman MS et al. Intensive Care Med 2012]. Aerosolization can also improve diffusion into the alveolar compartment compared with IV use [Luyt CE et al. Crit Care 2009]. There is limited data to support aerosolized antibiotic use in the ICU. One study showed no additional benefit of adding aerosolized antibiotic to IV antibiotics. Clinical cure rate was higher in aerosol treated patients (p=0.05; Figure 1) but not clinical success, eradication, or all-cause mortality [Kofteridis DP et al. Clin Infect Dis 2010].
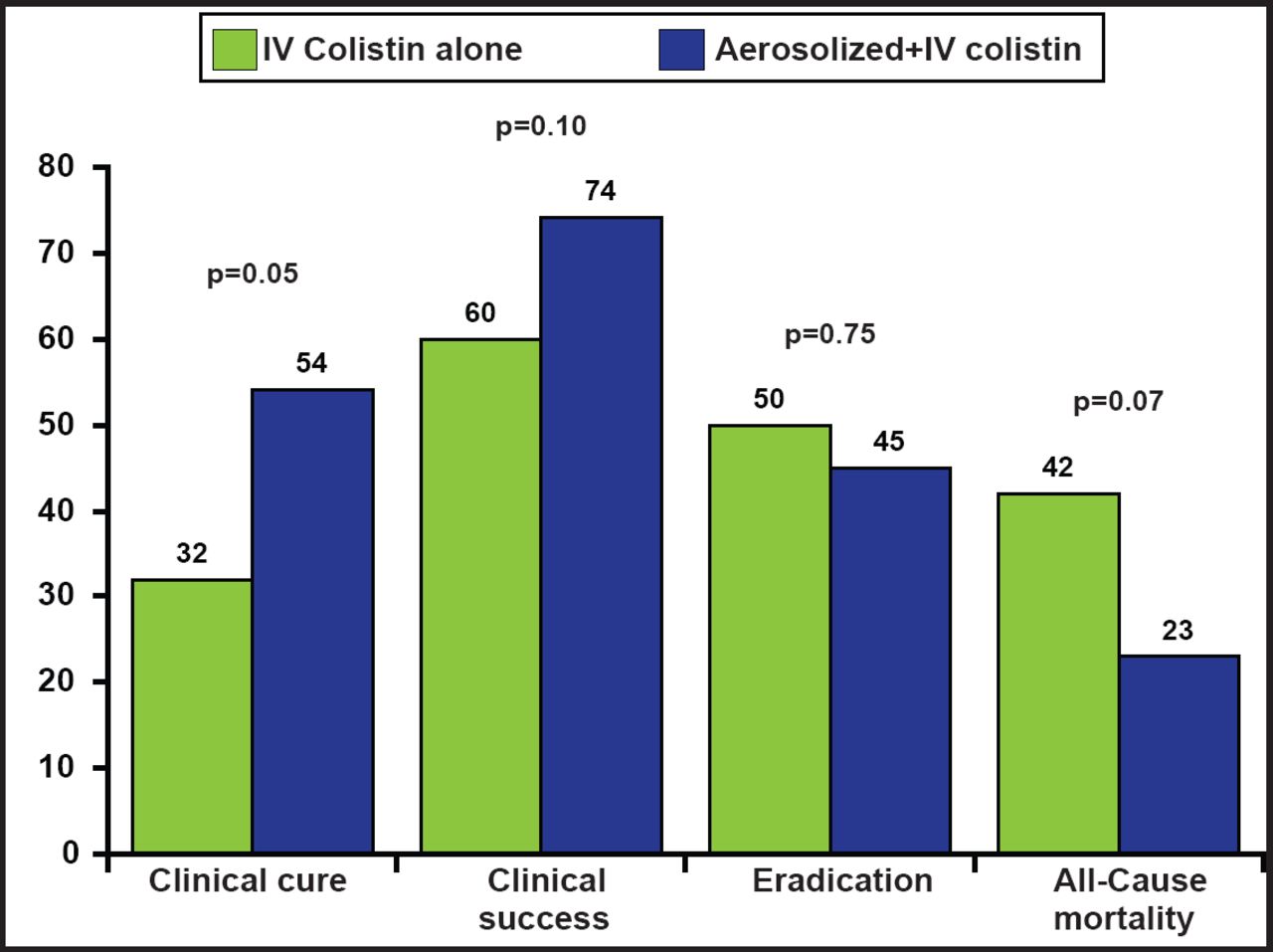
Aerosolized plus IV Colisitin Versus IV Colisitin Alone for the Treatment of VAP: A Matched Case-Control Study.
Reprinted with permission from the American Society for Microbiology. Kofteridis DP et al. Aerosolized plus intravenous colistin versus intravenous colistin alone for the treatment of ventilator-associated pneumonia: A matched case-control study. Clin Infect Dis. 2010;51(11):1238–44.
Although experimental and clinical studies clearly demonstrate nebulization can markedly increase the delivery of antibiotics to the deep lung, convincing clinical data based on large randomized trials are still lacking to support the routine administration of nebulized antibiotics for treating VAP.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.